

Etiologic spectrum and occurrence of coinfections in children hospitalized with community-acquired pneumonia
- PMID: 29262797
- PMCID: PMC5738861
- DOI: 10.1186/s12879-017-2891-x
Etiologic spectrum and occurrence of coinfections in children hospitalized with community-acquired pneumonia
Abstract
Background: Co-infections are common in childhood community acquired pneumonia (CAP). However, their etiological pattern and clinical impact remains inconclusive.
Methods: Eight hundred forty-six consecutive children with CAP were evaluated prospectively for the presence of viral and bacterial pathogens. Nasopharyngeal aspirates were examined by direct immunofluorescence assay or polymerase chain reaction (PCR) for viruses. PCR of nasopharyngeal aspirates and enzyme-linked immunosorbent assays were performed to detect M. pneumoniae. Bacteria was detected in blood, bronchoalveolar lavage specimen, or pleural fluid by culture.
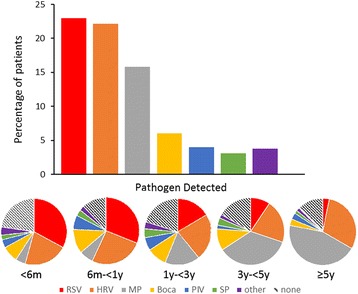
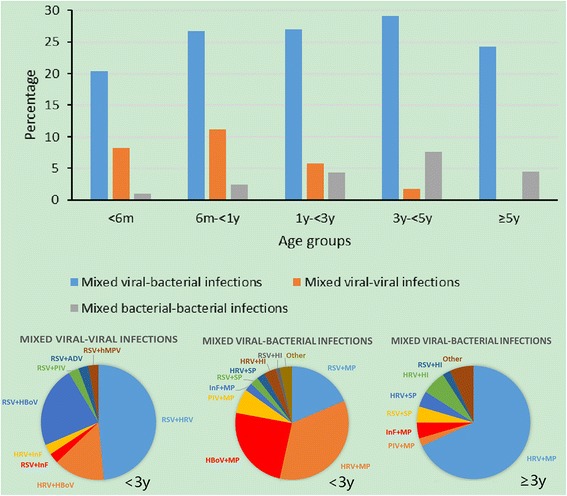
Results: Causative pathogen was identified in 70.1% (593 of 846) of the patients. The most commonly detected pathogens were respiratory syncytial virus (RSV) (22.9%), human rhinovirus (HRV) (22.1%), M. pneumoniae (15.8%). Coinfection was identified in 34.6% (293 of 846) of the patients. The majority of these (209 [71.3%] of 293) were mixed viral-bacterial infections. Age < 6 months (odds ratio: 2.1; 95% confidence interval: 1.2-3.3) and admission of PICU (odds ratio: 12.5; 95% confidence interval: 1.6-97.4) were associated with mix infection. Patients with mix infection had a higher rate of PICU admission.
Conclusions: The high mix infection burden in childhood CAP underscores a need for the enhancement of sensitive, inexpensive, and rapid diagnostics to accurately identify pneumonia pathogens.
Keywords: Children; Coinfection; Community-acquired pneumonia.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the Medical Ethics Committee of Children’s Hospital of Soochow University. The parents of all study participants gave written informed consent before study enrollment.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Nair H, Simoes EA, Rudan I, Gessner BD, Azziz-Baumgartner E, Zhang JS, et al. Global and regional burden of hospital admissions for severe acute lower respiratory infections in young children in 2010: a systematic analysis. Lancet. 2013;381:1380–1390. doi: 10.1016/S0140-6736(12)61901-1. - DOI - PMC - PubMed
-
- Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, et al. Executive summary: the management of community-acquired pneumonia in infants and children older than 3 months of age: clinical practice guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America. Clin Infect Dis. 2011;53:617–630. doi: 10.1093/cid/cir625. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
