

Arteriovenous fistulae after renal biopsy: diagnosis and outcomes using Doppler ultrasound assessment
- PMID: 29262805
- PMCID: PMC5738109
- DOI: 10.1186/s12882-017-0786-0
Arteriovenous fistulae after renal biopsy: diagnosis and outcomes using Doppler ultrasound assessment
Abstract
Background: Percutaneous renal biopsy (PRB) is an important technique providing relevant information to guide diagnosis and treatment in renal disease. As an invasive procedure it has complications. Most studies up to date have analysed complications related to bleeding. We report the largest single-center experience on routine Doppler ultrasound (US) assessment post PRB, showing incidence and natural history of arteriovenous fistulae (AVF) post PRB.
Methods: We retrospectively analysed 327 consecutive adult PRB performed at Ramon Cajal University Hospital between January 2011 and December 2014. All biopsies were done under real-time US guidance by a trained nephrologist. Routine Doppler mapping and kidney US was done within 24 h post biopsy regardless of symptoms. Comorbidities, full blood count, clotting, bleeding time and blood pressure were recorded at the time of biopsy. Post biopsy protocol included vitals and urine void checked visually for haematuria. Logistic regression was used to investigate links between AVF, needle size, correcting for potential confounding variables.
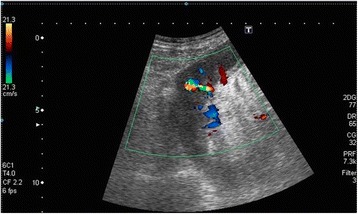
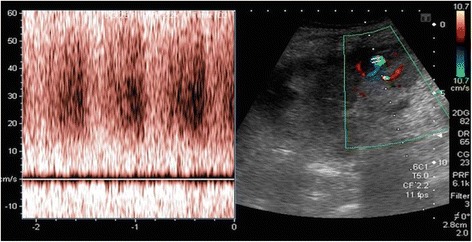
Results: 46,5% were kidney transplants and 53,5% were native biopsies. Diagnostic material was obtained in 90,5% (142 grafts and 154 native). Forty-seven AVF's (14.37%) were identified with routine kidney Doppler mapping, 95% asymptomatic (n = 45), 28 in grafts (18.4%) and 17 natives (9.7%) (p-value 0.7). Both groups were comparable in terms of comorbidities, passes, cylinders or biopsy yield (p-value NS). 80% were <1 cm in size and 46.6% closed spontaneously in less than 30 days (range 3-151). Larger AVF's (1-2 cm) took a mean of 52 days to closure (range 13-151). Needle size was not statistically significant factor for AVF (p-value 0.71).
Conclusions: Contrary to historical data published, AVF's are a common complication post PRB that can be easily missed. Routine US Doppler mapping performed by trained staff is a cost-effective, non-invasive tool to diagnose and follow up AVF's, helping to assess management.
Keywords: Arteriovenous fistula; Diagnostic and interventional nephrology; Doppler scan; Post biopsy complication; Renal biopsy; Renal ultrasound.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the Institutional Review Board at University Hospital Ramon y Cajal (reference 026/17). As collected data were obtained from routine clinical practice further consents were waived.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Richards NT, et al. Knowledge of renal histology alters patient management in over 40% of cases. Nephrol Dial Transplant. 1994;9(9):1255–9. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
