

Randomized Clinical Trial of Standard- Versus High-Calorie Formula for Methadone-Exposed Infants: A Feasibility Study
- PMID: 29263124
- PMCID: PMC5744267
- DOI: 10.1542/hpeds.2017-0114
Randomized Clinical Trial of Standard- Versus High-Calorie Formula for Methadone-Exposed Infants: A Feasibility Study
Abstract
Background: Newborns who are prenatally exposed to methadone are at risk for neonatal abstinence syndrome and the associated excess weight loss and poor weight gain. This pilot feasibility study aimed to evaluate early caloric enhancement on weight patterns among infants born to women receiving methadone maintenance therapy while pregnant.
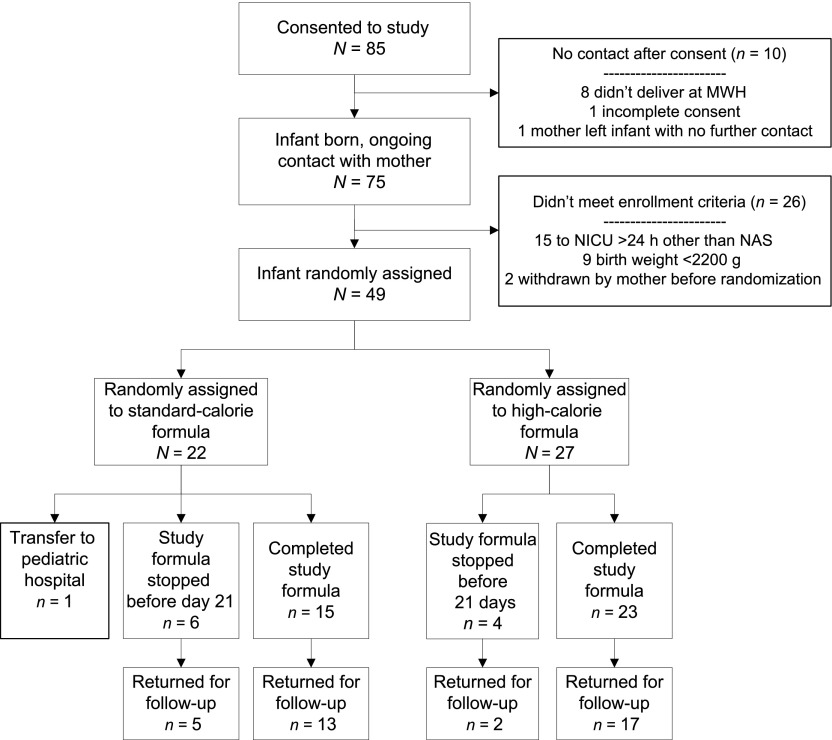
Methods: In this double-blind pilot feasibility study, we randomly assigned infants with fetal methadone exposure to 24 or 20 kcal/oz formula from days 3 to 21. Randomization was stratified by any breastfeeding, sex of the infant, and gestational age. Eligible infants were ≥35 weeks' gestation and weighed ≥2200 g. Outcomes were days to weight nadir, maximum percent weight loss, days to birth weight, percentage weight change per day, and feasibility.
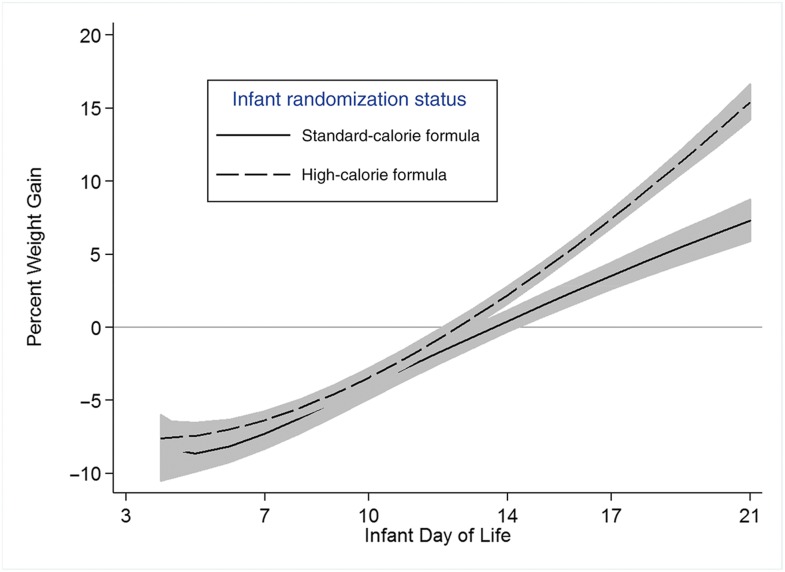
Results: A total of 49 infants were randomly assigned (22 to standard- and 27 to high-calorie formula); groups had comparable demographic characteristics. Main outcomes comparing standard- to high-calorie formula groups were not significant (days to weight nadir, 5.0 vs 4.4 days; P = .20; maximum percent weight loss, -9.4% vs -8.6%; P = .15; days to birth weight, 14.7 vs 13.6 days; P = .07); however, in longitudinal analyses (days 4 to 21), the high-calorie group had a higher percent weight gained per day compared with the standard-calorie group (P <.001). There were high levels of protocol adherence, and no adverse effects were observed.
Conclusions: Study findings suggest that early initiation of high-calorie formula for infants with prenatal methadone exposure may be beneficial for weight gain; evaluation in a larger study is warranted.
Copyright © 2018 by the American Academy of Pediatrics.
Conflict of interest statement
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
Figures
Comment in
-
Neonatal Abstinence Syndrome and the Pediatric Hospitalist: 5 Years Later.Hosp Pediatr. 2018 Jan;8(1):51-52. doi: 10.1542/hpeds.2017-0216. Hosp Pediatr. 2018. PMID: 29263123 No abstract available.
References
-
- Patrick SW, Schumacher RE, Benneyworth BD, Krans EE, McAllister JM, Davis MM. Neonatal abstinence syndrome and associated health care expenditures: United States, 2000-2009. JAMA. 2012;307(18):1934–1940 - PubMed
-
- Tolia VN, Patrick SW, Bennett MM, et al. Increasing incidence of the neonatal abstinence syndrome in U.S. neonatal ICUs. N Engl J Med. 2015;372(22):2118–2126 - PubMed
-
- Arlettaz R, Kashiwagi M, Das-Kundu S, Fauchère JC, Lang A, Bucher HU. Methadone maintenance program in pregnancy in a Swiss perinatal center (II): neonatal outcome and social resources. Acta Obstet Gynecol Scand. 2005;84(2):145–150 - PubMed
-
- Lifshitz M, Gavrilov V, Galil A, Landau D. A four year survey of neonatal narcotic withdrawal: evaluation and treatment. Isr Med Assoc J. 2001;3(1):17–20 - PubMed
-
- Maas U, Kattner E, Weingart-Jesse B, Schäfer A, Obladen M. Infrequent neonatal opiate withdrawal following maternal methadone detoxification during pregnancy. J Perinat Med. 1990;18(2):111–118 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
