

Pulmonary arterial hypertension: tailoring treatment to risk in the current era
- PMID: 29263175
- PMCID: PMC9488605
- DOI: 10.1183/16000617.0095-2017
Pulmonary arterial hypertension: tailoring treatment to risk in the current era
Abstract
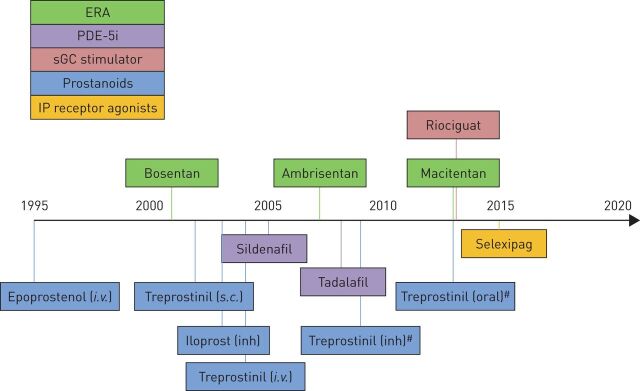
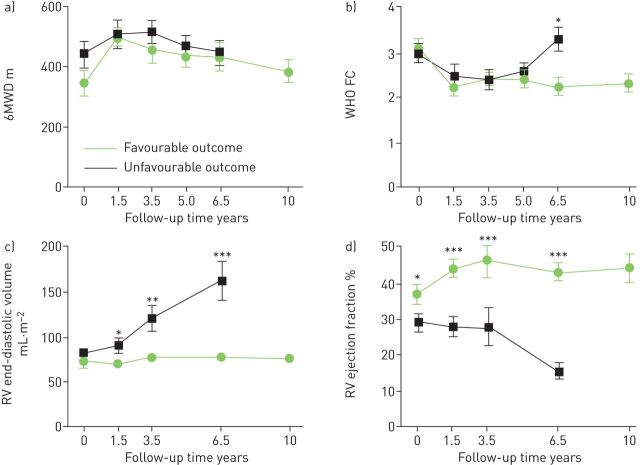
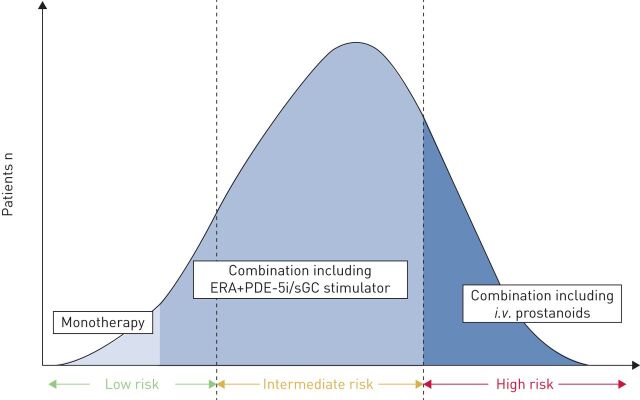
Recent advances in the treatment of pulmonary arterial hypertension (PAH) have led to improved patient outcomes. Multiple PAH therapies are now available and optimising the use of these drugs in clinical practice is vital. In this review, we discuss the management of PAH patients in the context of current treatment guidelines and supporting clinical evidence. In clinical practice, considerable emphasis is placed on the importance of making treatment decisions guided by each patient's risk status, which should be assessed using multiple prognostic parameters. As PAH is a progressive disease, regular assessments are essential to ensure that any change in risk is detected in a timely manner and treatment is adjusted accordingly. With the availability of therapies that target three different pathogenic pathways, combination therapy is now the standard of care. For most patients, this involves dual combination therapy with agents targeting the endothelin and nitric oxide pathways. Therapies targeting the prostacyclin pathway should be added for patients receiving dual combination therapy who do not achieve a low-risk status. There is also a need for a holistic approach to treatment beyond pharmacological therapies. Implementation of all these approaches will ensure that PAH patients receive maximal benefit from currently available therapies.
Copyright ©ERS 2017.
Conflict of interest statement
Conflict of interest: Disclosures can be found alongside this article at err.ersjournals.com
Figures
Comment in
References
-
- Humbert M, Lau EM, Montani D, et al. Advances in therapeutic interventions for patients with pulmonary arterial hypertension. Circulation 2014; 130: 2189–2208. - PubMed
-
- US Food and Drug Administration (FDA). FDA Approved Drug Products. www.accessdata.fda.gov/scripts/cder/daf/ Date last accessed: August 2017. Date last updated: August 2017.
-
- United Therapeutics. United Therapeutics Receives FDA Approval for REMODULIN™ to Treat Pulmonary Arterial Hypertension. www.sec.gov/Archives/edgar/data/1082554/000095013302002150/w61118exv99.htm Date last accessed: August 2017. Date last updated: May 2002.
-
- United Therapeutics. FDA Approves Intravenous Dosing of REMODULIN® for the Treatment of Pulmonary Arterial Hypertension. http://files.shareholder.com/downloads/UTHR/4970422123×0×63346/159F2EED-... Date last accessed: August 2017. Date last updated: November 2004.
-
- European Medicines Agency. European Public Assessment Reports.www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/landing/epar_search... Date last accessed: August 2017. Date last updated: August 2017.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials