

The Cost of Hematopoietic Stem-Cell Transplantation in the United States
- PMID: 29263771
- PMCID: PMC5726064
The Cost of Hematopoietic Stem-Cell Transplantation in the United States
Abstract
Background: Hematopoietic stem-cell transplantation (HSCT) requires highly specialized, resource-intensive care. Myeloablative conditioning regimens used before HSCT generally require inpatient stays and are more intensive than other preparative regimens, and may therefore be more costly.
Objective: To estimate the costs associated with inpatient HSCT according to the type of the conditioning regimen used and other potential contributors to the overall cost of the procedure.
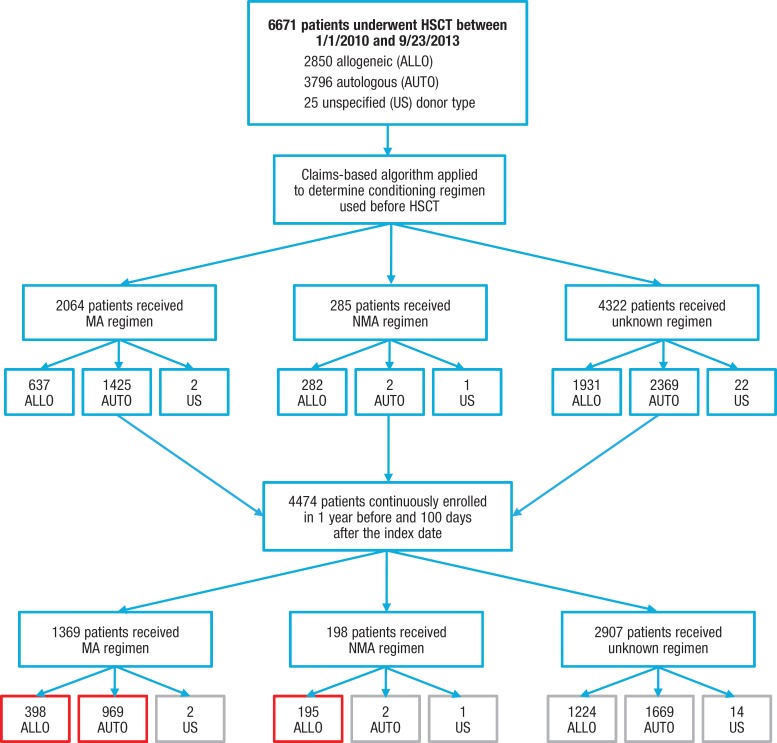
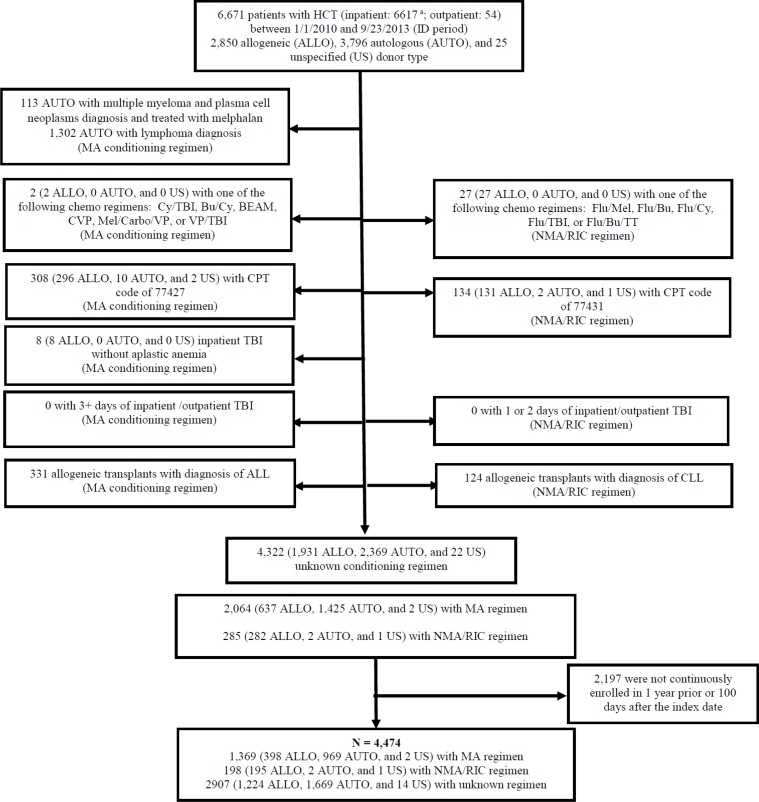
Method: We used data from the Truven Health MarketScan insurance claims database to analyze healthcare costs for pediatric (age <18 years) and adult (age ≥18 years) patients who had autologous or allogeneic inpatient HSCT between January 1, 2010, and September 23, 2013. We developed an algorithm to determine whether conditioning regimens were myeloablative or nonmyeloablative/reduced intensity.
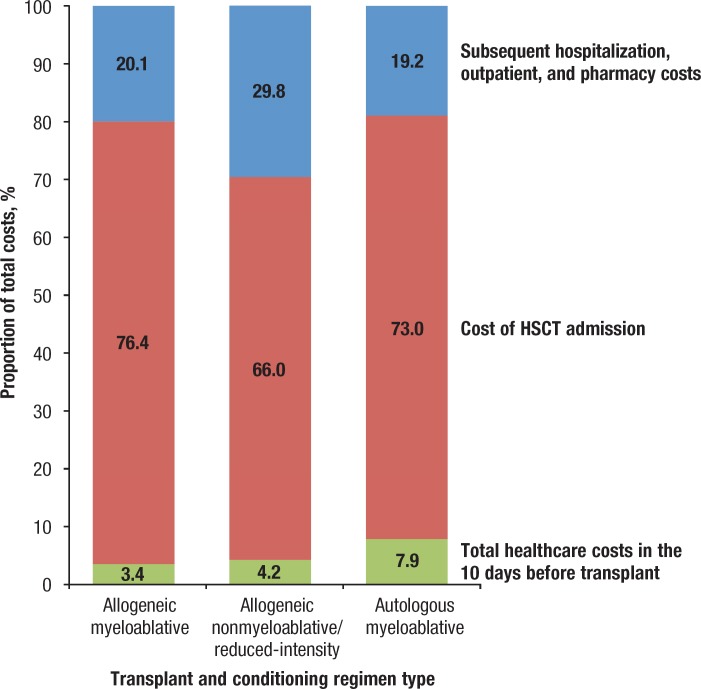
Results: We identified a sample of 1562 patients who had inpatient HSCT during the study period for whom the transplant type and the conditioning regimen were determinable: 398 patients had myeloablative allogeneic HSCT; 195 patients had nonmyeloablative/reduced-intensity allogeneic HSCT; and 969 patients had myeloablative autologous HSCT. The median total healthcare cost at 100 days was $289,283 for the myeloablative allogeneic regimen cohort compared with $253,467 for the nonmyeloablative/reduced-intensity allogeneic regimen cohort, and $140,792 for the myeloablative autologous regimen cohort. The mean hospital length of stay for the index (first claim of) HSCT was 35.6 days in the myeloablative allogeneic regimen cohort, 26.6 days in the nonmyeloablative/reduced-intensity allogeneic cohort, and 21.8 days in the myeloablative autologous regimen cohort.
Conclusion: Allogeneic HSCT was more expensive than autologous HSCT, regardless of the regimen used. Myeloablative conditioning regimens led to higher overall costs than nonmyeloablative/reduced-intensity regimens in the allogeneic HSCT cohort, indicating a greater cost burden associated with inpatient services for higher-intensity preparative conditioning regimens. Pediatric patients had higher costs than adult patients. Future research should involve validating the algorithm for identifying conditioning regimens using clinical data.
Keywords: allogeneic HSCT; autologous HSCT; healthcare costs; hospitalization; inpatient; myeloablative conditioning regimen; nonmyeloablative/reduced-intensity conditioning regimen.
Figures

References
-
- Pasquini MC, Zhu X. Current uses and outcomes of hematopoietic stem cell transplantation: CIBMTR Summary Slides, 2015. www.cibmtr.org/ReferenceCenter/SlidesReports/SummarySlides/Pages/index.aspx. Accessed September 15, 2015.
-
- Stranges E, Russo CA, Friedman B. Procedures with the most rapidly increasing hospital costs, 2004–2007. Healthcare Cost and Utilization Project statistical brief #82. December 2009. Agency for Healthcare Research and Quality; Rockville, MD. www.hcup-us.ahrq.gov/reports/statbriefs/sb82.jsp. Accessed March 16, 2016.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical