

A phase 3, double-blind, randomized placebo-controlled efficacy and safety study of abiraterone acetate in chemotherapy-naïve patients with mCRPC in China, Malaysia, Thailand and Russia
- PMID: 29264210
- PMCID: PMC5717983
- DOI: 10.1016/j.ajur.2017.01.002
A phase 3, double-blind, randomized placebo-controlled efficacy and safety study of abiraterone acetate in chemotherapy-naïve patients with mCRPC in China, Malaysia, Thailand and Russia
Abstract
Objective: This double-blind, placebo-controlled phase 3 study was designed to compare efficacy and safety of abiraterone acetate + prednisone (abiraterone) to prednisone alone in chemotherapy-naïve, asymptomatic or mildly symptomatic metastatic castration-resistant prostate cancer (mCRPC) patients from China, Malaysia, Thailand and Russia.
Methods: Adult chemotherapy-naïve patients with confirmed prostate adenocarcinoma, Eastern Cooperative Oncology Group (ECOG) performance status (PS) grade 0-1, ongoing androgen deprivation (serum testosterone <50 ng/dL) with prostate specific antigen (PSA) or radiographic progression were randomized to receive abiraterone acetate (1000 mg, QD) + prednisone (5 mg, BID) or placebo + prednisone (5 mg, BID), until disease progression, unacceptable toxicity or consent withdrawal. Primary endpoint was improvements in time to PSA progression (TTPP).
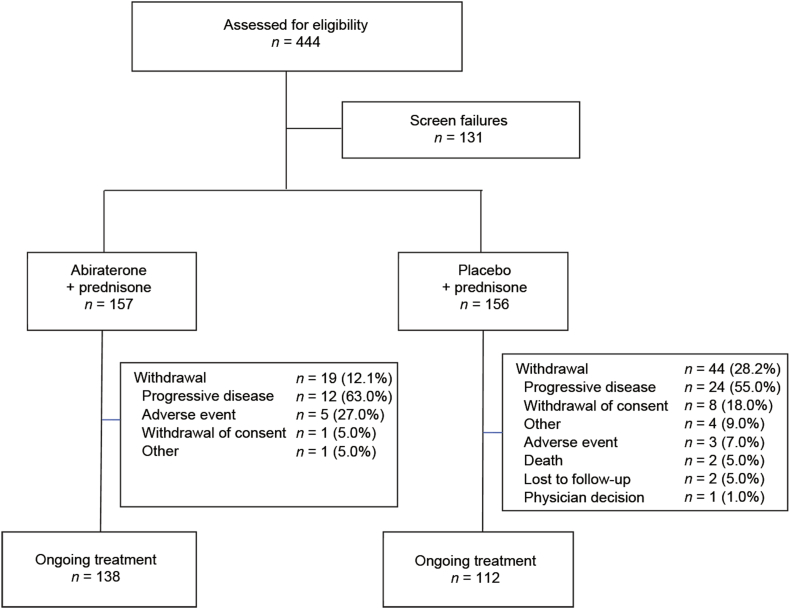
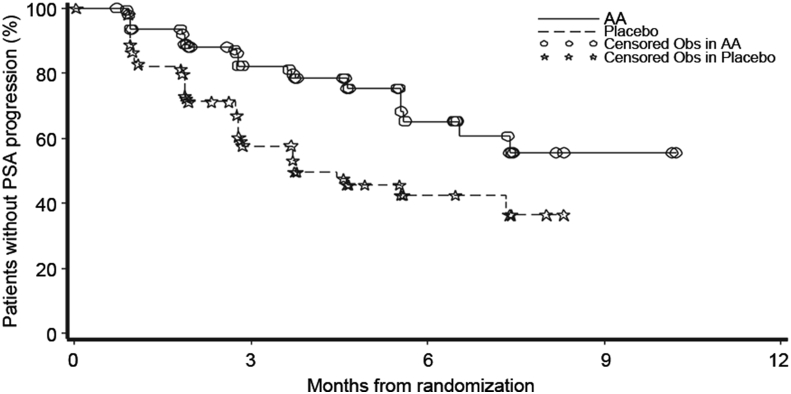
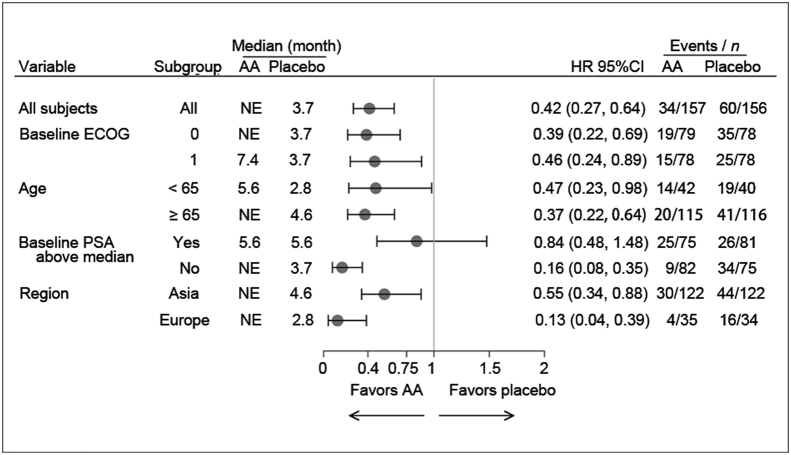
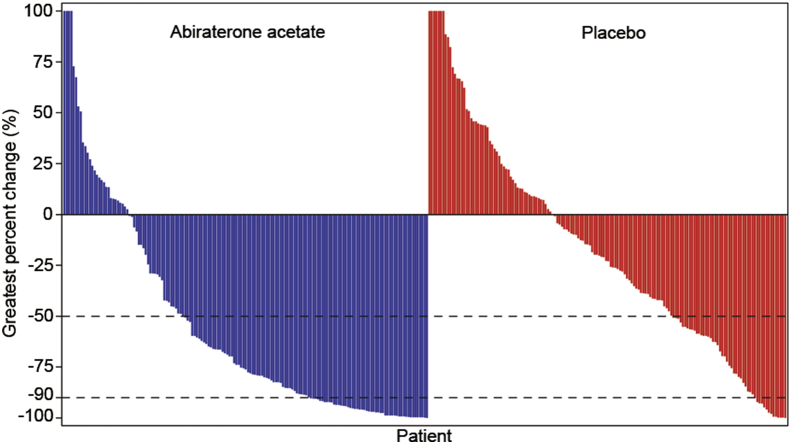
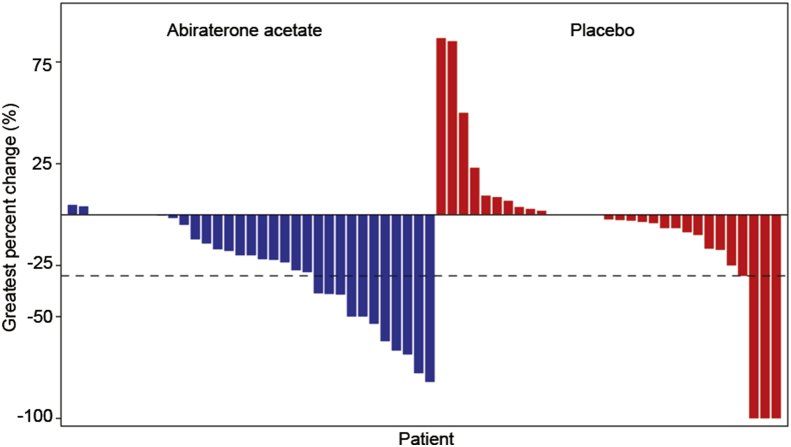
Results: Totally, 313 patients were randomized (abiraterone: n = 157; prednisone: n = 156); and baseline characteristics were balanced. At clinical cut-off (median follow-up time: 3.9 months), 80% patients received treatment (abiraterone: n = 138, prednisone: n = 112). Median time to PSA progression was not reached with abiraterone versus 3.8 months for prednisone, attaining 58% reduction in PSA progression risk (HR = 0.418; p < 0.0001). Abiraterone-treated patients had higher confirmed PSA response rate (50% vs. 21%; relative odds = 2.4; p < 0.0001) and were 5 times more likely to achieve radiographic response than prednisone-treated patients (22.9% vs. 4.8%, p = 0.0369). Median survival was not reached. Most common (≥10% abiraterone vs. prednisone-treated) adverse events: bone pain (7% vs. 14%), pain in extremity (6% vs. 12%), arthralgia (10% vs. 8%), back pain (7% vs. 11%), and hypertension (15% vs. 14%).
Conclusion: Interim analysis confirmed favorable benefit-to-risk ratio of abiraterone in chemotherapy-naïve men with mCRPC, consistent with global study, thus supporting use of abiraterone in this patient population.
Keywords: Abiraterone; Chemotherapy-naïve; Metastatic castration-resistant prostate cancer; Prednisone; Prostate specific antigen.
Figures
References
-
- GLOBOCAN 2012: estimated cancer incidence, mortality and prevalence worldwide in 2012. International Agency for Research in Cancer, World Health Organisation; 2012. http://globocan.iarc.fr/Pages/fact_sheets [20 Oct 2014]. Available from:
-
- Hoedemaeker R.F., Rietbergen J.B., Kranse R., Schroder F.H., van der Kwast T.H. Histopathological prostate cancer characteristics at radical prostatectomy after population based screening. J Urol. 2000;164:411–415. - PubMed
-
- Peyromaure M., Debre B., Mao K., Zhang G., Wang Y., Sun Z. Management of prostate cancer in China: a multicenter report of 6 institutions. J Urol. 2005;174:1794–1797. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
