

Perivascular Adductor Longus muscle injury: Ultrasound and Magnetic Resonance Imaging findings
- PMID: 29264350
- PMCID: PMC5725188
- DOI: 10.11138/mltj/2017.7.2.376
Perivascular Adductor Longus muscle injury: Ultrasound and Magnetic Resonance Imaging findings
Abstract
Background: Muscle injuries affecting the Adductor Longus are not all localised at the level of the proximal myotendinous junction and enthesis. Thus, the main purpose of this article was to raise awareness of the imaging features of the Perivascular Adductor Longus muscle injury, which currently remains widely under-recognised.
Methods: The ultrasound (US) and Magnetic Resonance imaging (MRI) images of five professional football players were retrospectively reassessed to identify distinctive imaging details of the Perivascular Adductor Longus muscle injury. Complementary information regarding the traumatic mechanics is presented as well.
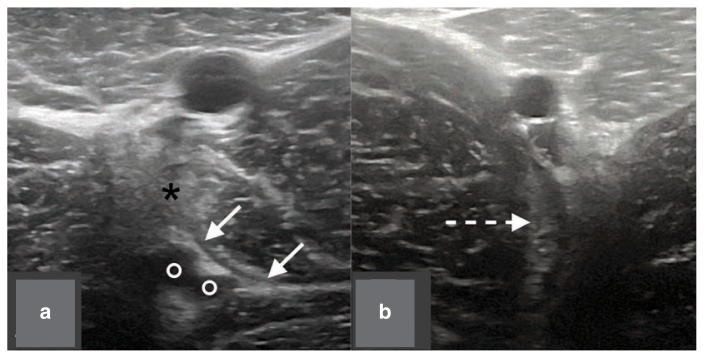
Results: All the players presented similar US images in the first seventy-two hours: loss of ecostructural integrity of the lateral epimysium, in proximity to the femoral vessels, and perilesional oedema were the main pathological findings. The injury lead to the formation of a hypoechoic, intramuscular haematoma in three of the subjects. Anyway, this was detectable only after five days, or later. Moreover, MRI sequences showed long-standing haematoma-related signal alterations which were also observable at three months after trauma. Typically, kicking was the traumatic motor task.
Conclusions: The main practical value of this technical note is to compensate for the lack of studies concerning the Perivascular Adductor Longus muscle injury. Promptly identifying its typical imaging features is crucial in order to establish the correct diagnosis and to implement a highly specific rehabilitative program.
Level of evidence: V.
Keywords: magnetic resonance imaging; soft tissue injuries; sports injuries; thigh; ultrasonography.
Conflict of interest statement
Conflict of interest The Authors declare that they have no conflict of interest.
Figures












References
-
- Dimitrakopoulou A, Schilders E, Bismil Q, Talbot JC, Kazakos K. An unusual case of enthesophyte formation following an adductor longus rupture in a high-level athlete. Knee Surg Sports Traumatol Arthrosc. 2010;18:691–693. - PubMed
-
- Serner A, Tol JL, Jomaah N, Weir A, Whiteley R, Thorborg K, et al. Diagnosis of Acute Groin Injuries: a prospective study of 110 athletes. Am J Sports Med. 2015;43(8):1857–1864. - PubMed
-
- Charnock BL, Lewis CL, Garrett JRWE, Queen RM. Adductor longus mechanics during the maximal effort soccer kick. Sports Biomech. 2009;8(3):223–234. - PubMed
-
- Pesquer L, Reboul G, Silvestre A, Poussange N, Meyer P, Dallaudière B. Imaging of adductor-related groin pain. Diagn Interv Imaging. 2015;96:861–869. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials