

Cabergoline Tapering Is Almost Always Successful in Patients With Macroprolactinomas
- PMID: 29264479
- PMCID: PMC5686686
- DOI: 10.1210/js.2017-00038
Cabergoline Tapering Is Almost Always Successful in Patients With Macroprolactinomas
Abstract
Context: Cabergoline (CAB) is very effective in the treatment of macroprolactinomas, but there are few data on the CAB dose necessary to achieve and maintain normal prolactin (PRL) levels.
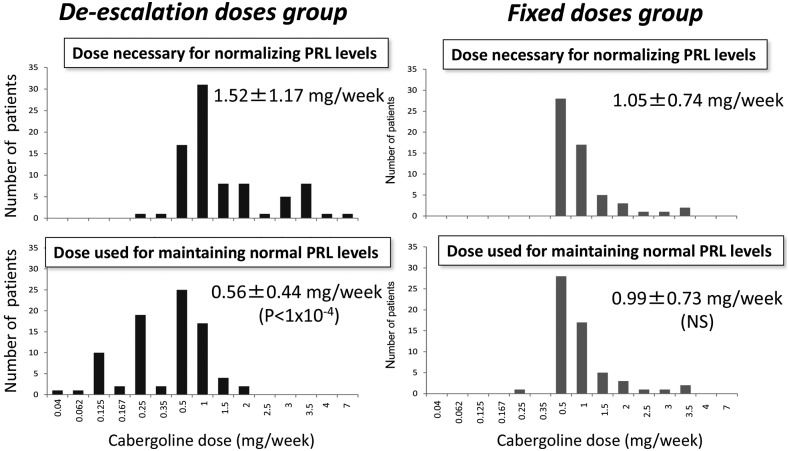
Design and patients: We retrospectively studied 260 patients. CAB was introduced at a mean dose of 0.83 ± 0.52 mg/wk. When the PRL level had normalized, the patient's physician chose to either maintain the CAB dose (fixed-dose group) or to taper it (de-escalation group) until the minimal effective dose required to maintain a normal PRL level was established.
Results: PRL normalized in 157 patients (60.8%) during CAB treatment. CAB de-escalation was attempted in 84 (53.5%) of these 157 patients and was successful in 77 (91.7%) cases. The mean CAB dose was reduced from 1.52 ± 1.17 mg/wk to 0.56 ± 0.44 mg/wk at the last visit (P < 1 × 10-4). De-escalation was also possible in some "CAB-resistant" patients, namely those requiring ≥2 mg/wk to normalize PRL. CAB de-escalation had no negative long-term effect on tumor size. At the last visit, maximal diameter was 8.8 ± 8.8 mm in the de-escalation group and 13.4 ± 8.5 mm in the fixed-dose group (P < 0.01).
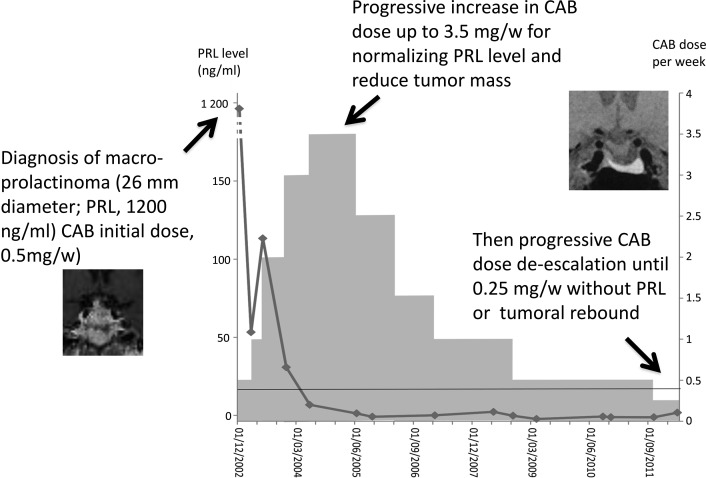
Conclusion: In patients with macroprolactinomas, the CAB dosage required to maintain a normal PRL level long term is lower than the initial dosage necessary to normalize the PRL level. After PRL normalization, CAB tapering was almost always successful, even when very high initial doses were necessary. CAB tapering does not undermine tumor control and may attenuate the potential adverse effects of CAB, which appear to be dependent on the cumulative dose.
Keywords: hyperprolactinemia; hypothalamus/pituitary; pituitary disease; prolactinoma.
Figures
References
-
- Bernard V, Young J, Chanson P, Binart N. New insights in prolactin: pathological implications. Nat Rev Endocrinol. 2015;11(5):265–275. - PubMed
-
- Chanson P, Maiter D. Prolactinoma. In: Melmed S, ed. The Pituitary. 4th ed. San Diego, CA: Elsevier; 2017:467–514.
-
- Casanueva FF, Molitch ME, Schlechte JA, Abs R, Bonert V, Bronstein MD, Brue T, Cappabianca P, Colao A, Fahlbusch R, Fideleff H, Hadani M, Kelly P, Kleinberg D, Laws E, Marek J, Scanlon M, Sobrinho LG, Wass JA, Giustina A. Guidelines of the Pituitary Society for the diagnosis and management of prolactinomas. Clin Endocrinol (Oxf). 2006;65(2):265–273. - PubMed
-
- Melmed S, Casanueva FF, Hoffman AR, Kleinberg DL, Montori VM, Schlechte JA, Wass JA; Endocrine Society . Diagnosis and treatment of hyperprolactinemia: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96(2):273–288. - PubMed
-
- Gillam MP, Molitch ME, Lombardi G, Colao A. Advances in the treatment of prolactinomas. Endocr Rev. 2006;27(5):485–534. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources