

Management of Asymptomatic Patients With Positive Coronary Artery Calcium Scans
- PMID: 29264512
- PMCID: PMC5689148
- DOI: 10.1210/js.2016-1080
Management of Asymptomatic Patients With Positive Coronary Artery Calcium Scans
Abstract
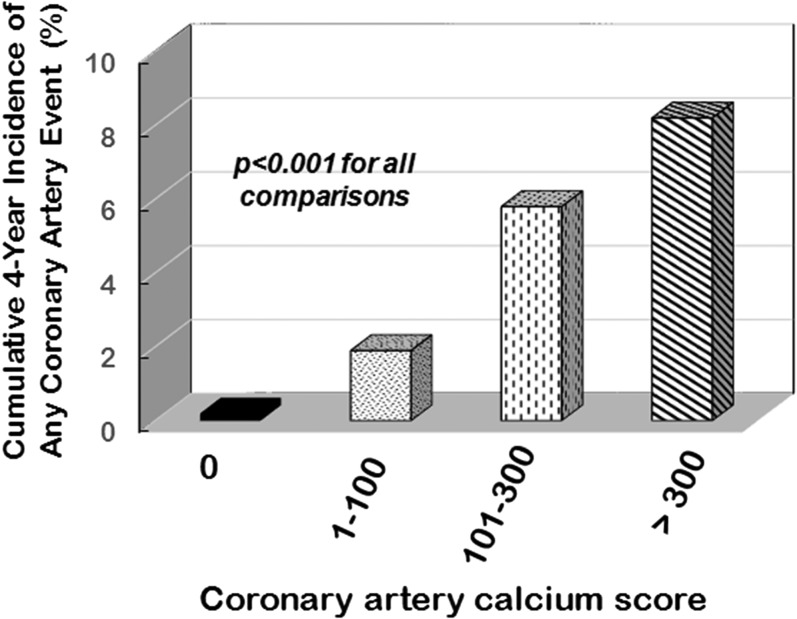
Background: The widespread availability of the coronary artery calcium scan to diagnose coronary artery atheroma semiquantitatively and its prognostic significance has frequently resulted in a difficult therapeutic decision for physicians caring for asymptomatic patients.
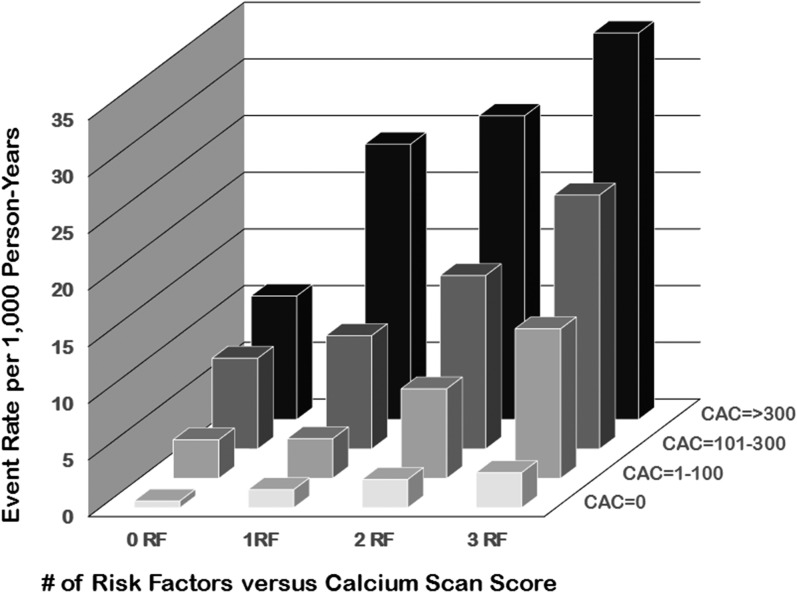
Patients and risk factors: Of particular concern are patients over 40 years of age and young adults characterized by multiple cardiovascular risk factors. The correct prognostic interpretation of coronary artery calcium scores and the potential benefits and risks of various therapeutic modalities need to be understood.
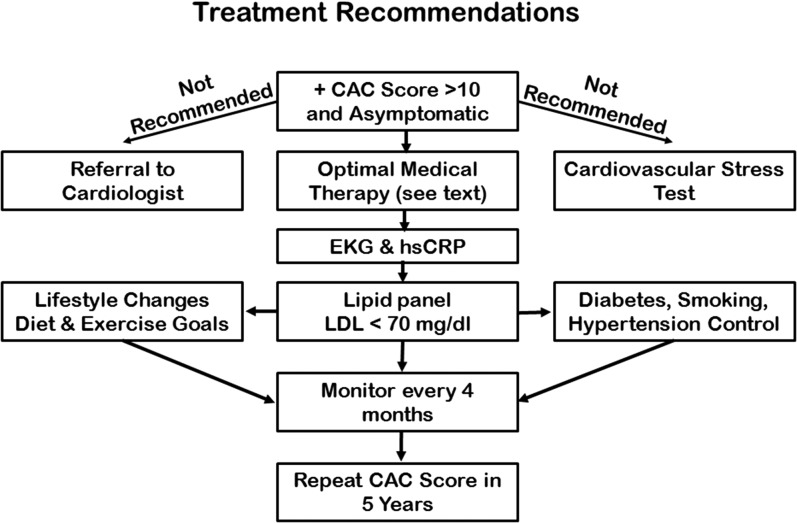
Conclusion: This review describes the therapeutic choices available to endocrinologists and provides recommendations for various treatment options.
Keywords: LDL cholesterol; calcium scan; coronary angiography; heart disease; statins; stress testing.
Figures
References
-
- McClelland RL, Jorgensen NW, Budoff M, Blaha MJ, Post WS, Kronmal RA, Bild DE, Shea S, Liu K, Watson KE, Folsom AR, Khera A, Ayers C, Mahabadi AA, Lehmann N, Jöckel KH, Moebus S, Carr JJ, Erbel R, Burke GL. 10-year coronary heart disease risk prediction using coronary artery calcium and traditional risk factors: derivation in the MESA (Multi-Ethnic Study of Atherosclerosis) with validation in the HNR (Heinz Nixdorf Recall) Study and the DHS (Dallas Heart Study). J Am Coll Cardiol. 2015;66(15):1643–1653. - PMC - PubMed
-
- Tota-Maharaj R, Blaha MJ, McEvoy JW, Blumenthal RS, Muse ED, Budoff MJ, Shaw LJ, Berman DS, Rana JS, Rumberger J, Callister T, Rivera J, Agatston A, Nasir K. Coronary artery calcium for the prediction of mortality in young adults <45 years old and elderly adults >75 years old. Eur Heart J. 2012;33(23):2955–2962. - PubMed
-
- Eaton RP, Burge MR, Comerci G, Cavanaugh B, Ramo B, Schade DS. Abnormal coronary artery calcium scans in asymptomatic patients. Am J Med. 2017;130(4):394–397. - PubMed
-
- Boden WE, O’Rourke RA, Teo KK, Hartigan PM, Maron DJ, Kostuk WJ, Knudtson M, Dada M, Casperson P, Harris CL, Chaitman BR, Shaw L, Gosselin G, Nawaz S, Title LM, Gau G, Blaustein AS, Booth DC, Bates ER, Spertus JA, Berman DS, Mancini GB, Weintraub WS; COURAGE Trial Research Group . Optimal medical therapy with or without PCI for stable coronary disease. N Engl J Med. 2007;356(15):1503–1516. - PubMed
-
- Sedlis SP, Hartigan PM, Teo KK, Maron DJ, Spertus JA, Mancini GBJ, Kostuk W, Chaitman BR, Berman D, Lorin JD, Dada M, Weintraub WS, Boden WE; COURAGE Trial Investigators . Effect of PCI on long-term survival in patients with stable ischemic heart disease. N Engl J Med. 2015;373(20):1937–1946. - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources