

Clopidogrel-Induced Insulin Autoimmune Syndrome: A Newly Recognized Cause of Hypoglycemia in a Patient Without Diabetes
- PMID: 29264578
- PMCID: PMC5686698
- DOI: 10.1210/js.2017-00316
Clopidogrel-Induced Insulin Autoimmune Syndrome: A Newly Recognized Cause of Hypoglycemia in a Patient Without Diabetes
Abstract
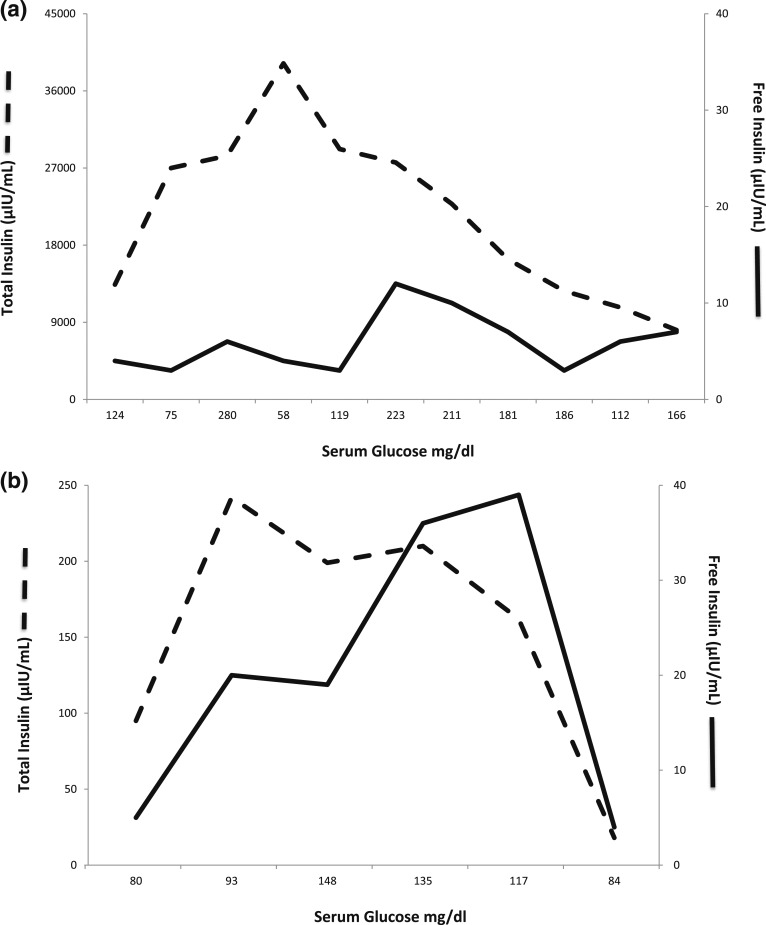
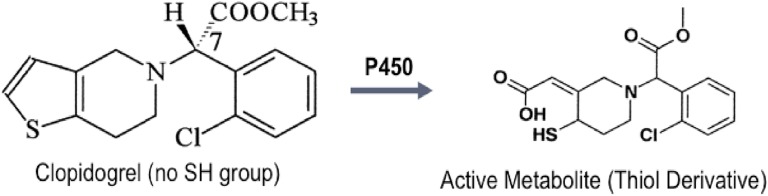
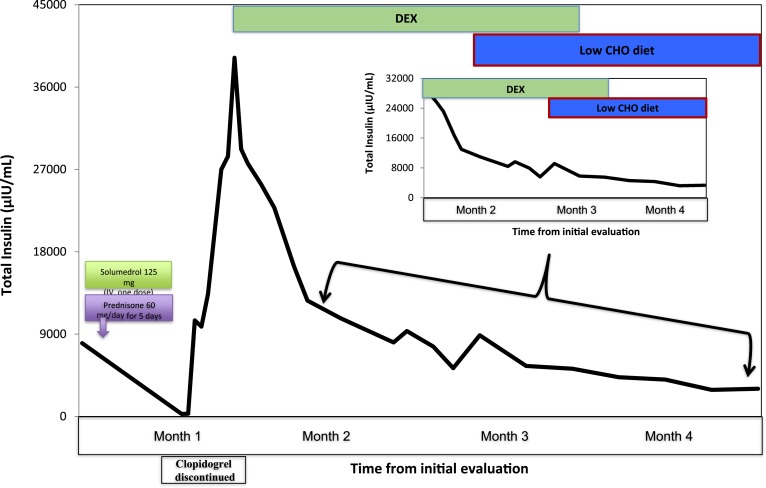
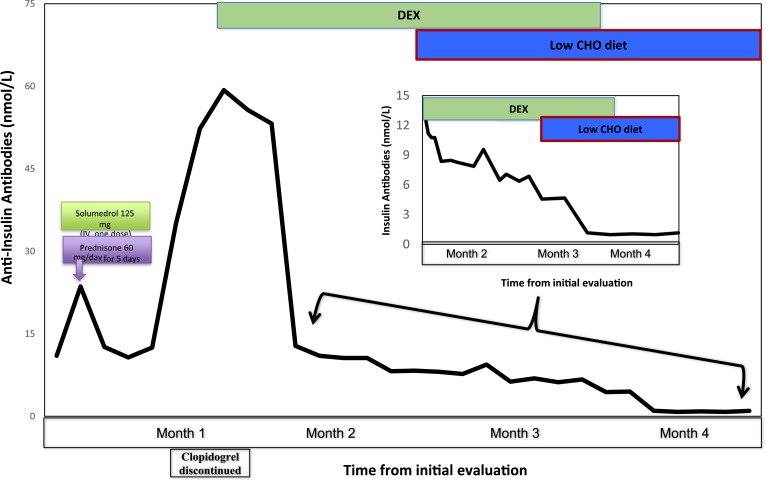
Insulin autoimmune syndrome (IAS), defined as hyperinsulinemic hypoglycemia with high titers of anti-insulin antibodies, is frequently reported in Japanese patients but rarely observed in whites. We report in this study on a 79-year-old white male without diabetes who developed IAS following exposure to clopidogrel, a drug not previously known to cause hypoglycemia. The patient presented with recurrent symptomatic hypoglycemia. During one episode, serum glucose was 45 mg/dL, whereas insulin and C-peptide levels were 40,000 mIU/mL and 40 ng/mL, respectively. Additional studies revealed no intake of insulin or its secretagogues, whereas anti-insulin antibody titer was high (59.3 nmol/L). Although total insulin levels were consistently high, free insulin concentrations (polyethylene glycol precipitation) were appropriate for ambient glycemia. The patient was found to have HLA-DRB1*0404, a feature often reported in Japanese patients with IAS. Three weeks prior to symptom onset, he was started on clopidogrel, a drug that does not have a sulfhydryl group, but its active metabolite does. Clopidogrel was switched to a nonsulfhydryl antiplatelet agent, and glucocorticoid therapy was initiated. Shortly thereafter, the frequency of hypoglycemic episodes decreased, and glucocorticoids were tapered over the ensuing 3 months. No hypoglycemic episodes were noted during 6 months of observation after discontinuing glucocorticoids, whereas the total insulin and anti-insulin antibody levels normalized. The data indicate that IAS should be considered in the differential diagnosis of hyperinsulinemic hypoglycemia in seemingly well individuals, even when no drugs known to cause IAS were used. Clinical suspicion of IAS can avoid expensive imaging and unnecessary surgery in affected patients.
Keywords: clopidogrel; drug-induced hypoglycemia; hypoglycemia; insulin autoimmune syndrome.
Figures
References
-
- Cryer PE, Axelrod L, Grossman AB, Heller SR, Montori VM, Seaquist ER, Service FJ; Endocrine Society . Evaluation and management of adult hypoglycemic disorders: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2009;94(3):709–728. - PubMed
-
- Lupsa BC, Chong AY, Cochran EK, Soos MA, Semple RK, Gorden P. Autoimmune forms of hypoglycemia. Medicine (Baltimore). 2009;88(3):141–153. - PubMed
-
- Hirata Y, Ishizu H, Ouchi N, Motomura M, Abe M, Hara Y, Wakasugi H, Takahashi L, Sakano H, Tanaka M, Kawano H, Kanesaki T. Insulin autoimmunity in a case of spontaneous hypoglycemia. J Jpn Diabetes Soc. 1970;13:312–320.
-
- Uchigata Y, Hirata Y. Insulin autoimmune syndrome (IAS, Hirata disease). Ann Med Interne (Paris). 1999;150(3):245–253. - PubMed
-
- Uchigata Y, Tokunaga K, Nepom G, Bannai M, Kuwata S, Dozio N, Benson EA, Ronningen KS, Spinas GA, Tadokoro K, Hirata Y, Juji T, Omori Y. Differential immunogenetic determinants of polyclonal insulin autoimmune syndrome (Hirata’s disease) and monoclonal insulin autoimmune syndrome. Diabetes. 1995;44(10):1227–1232. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials