

Anticoagulants Influence the Performance of In Vitro Assays Intended for Characterization of Nanotechnology-Based Formulations
- PMID: 29267243
- PMCID: PMC5943954
- DOI: 10.3390/molecules23010012
Anticoagulants Influence the Performance of In Vitro Assays Intended for Characterization of Nanotechnology-Based Formulations
Abstract
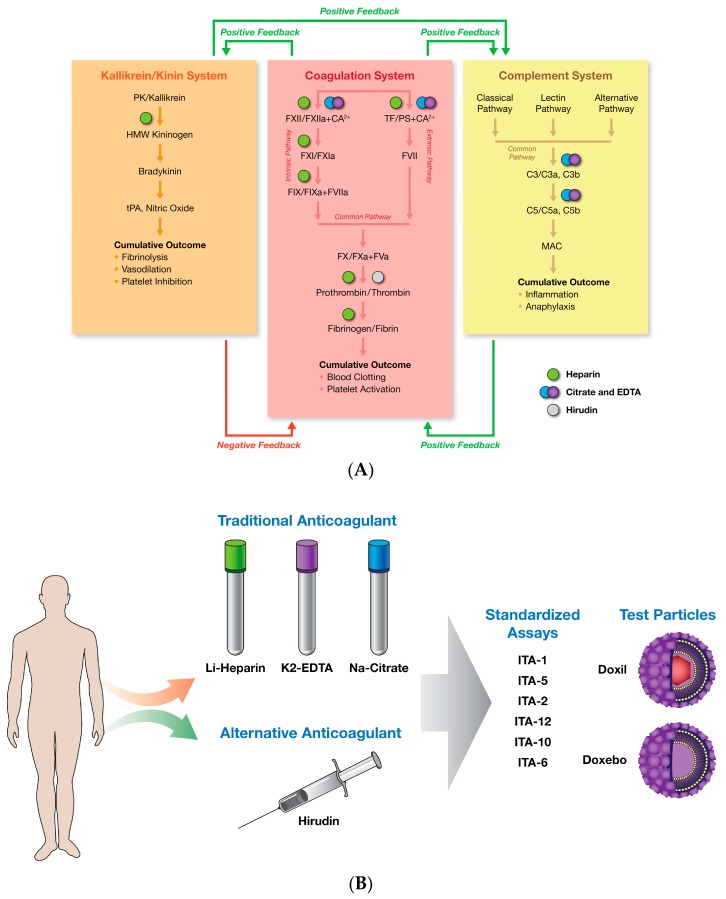
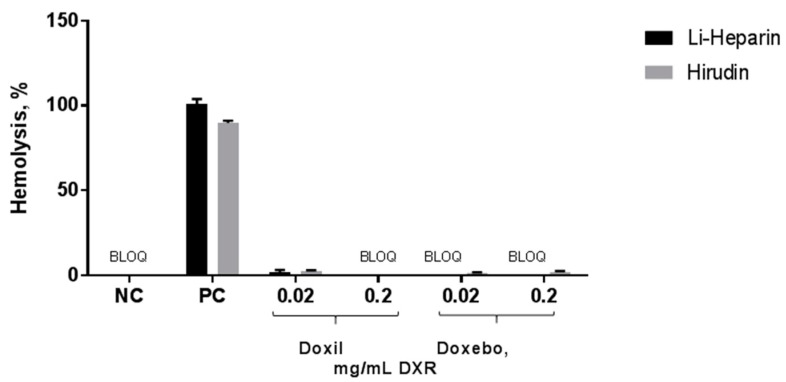
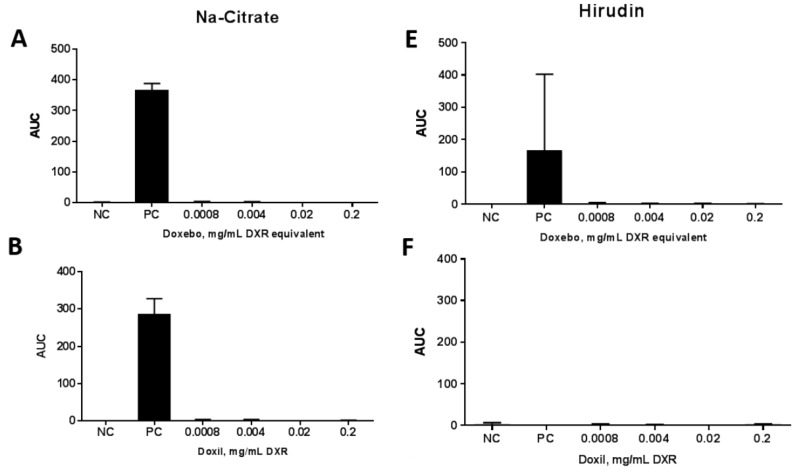
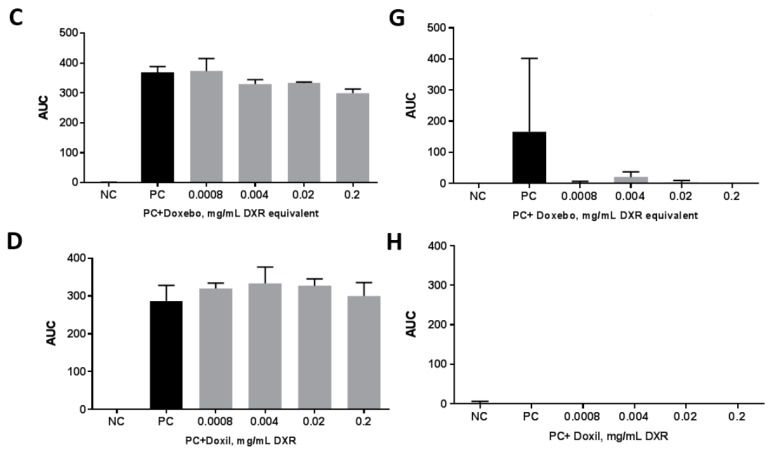
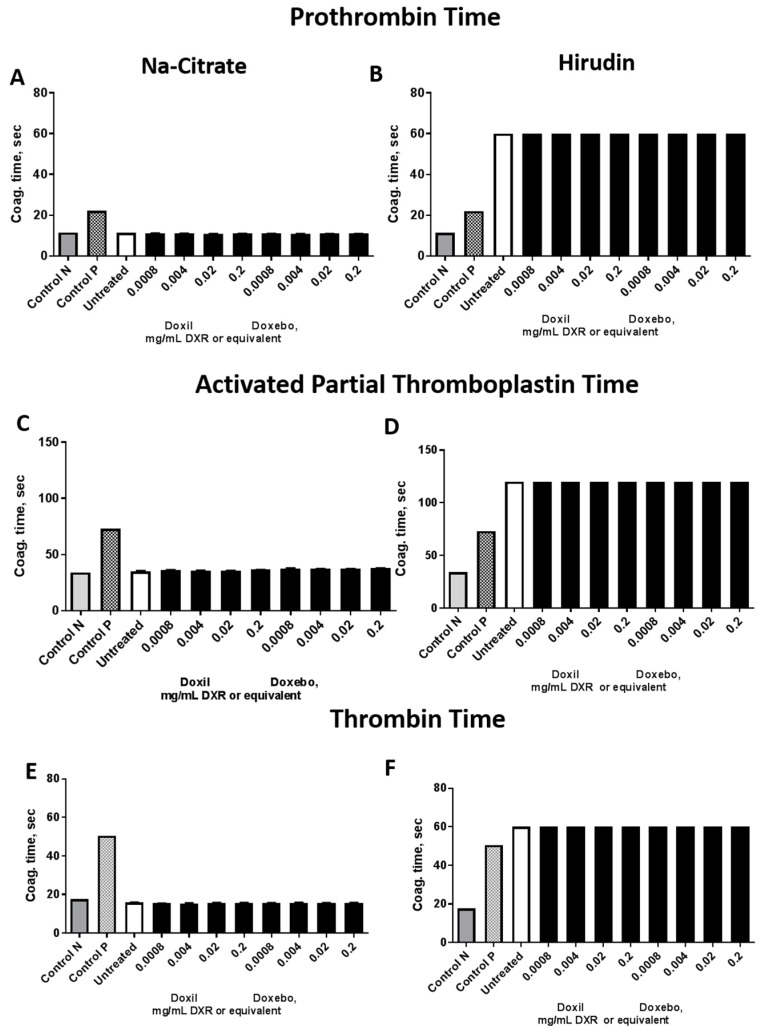
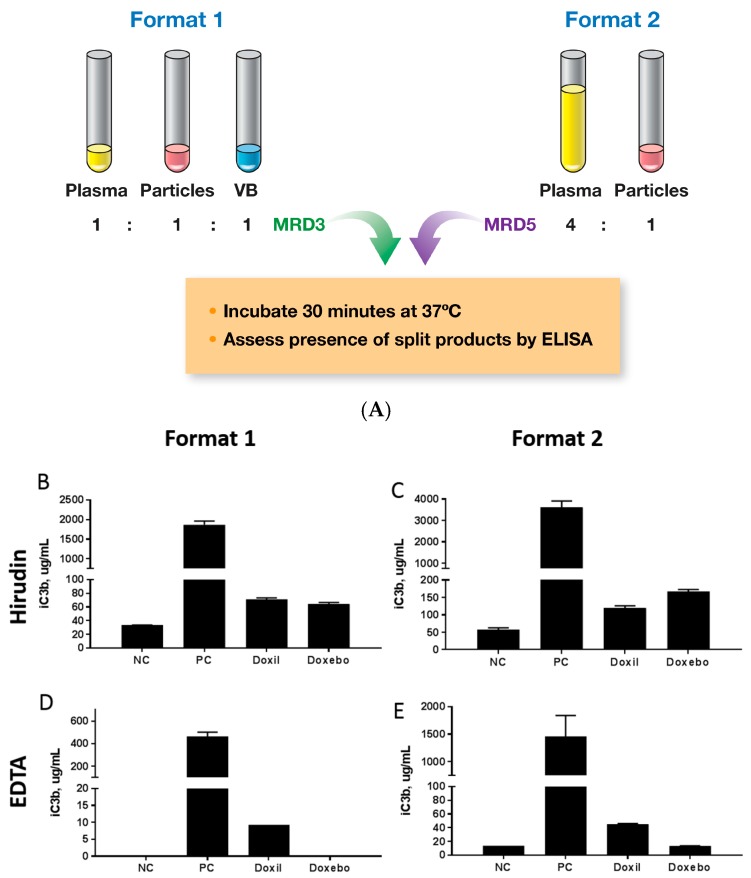
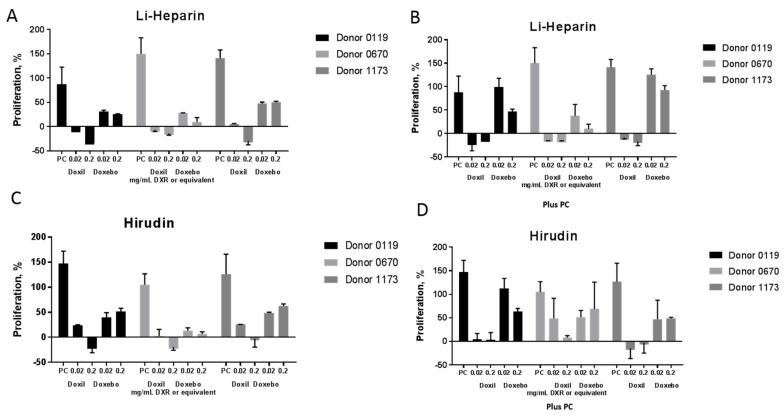
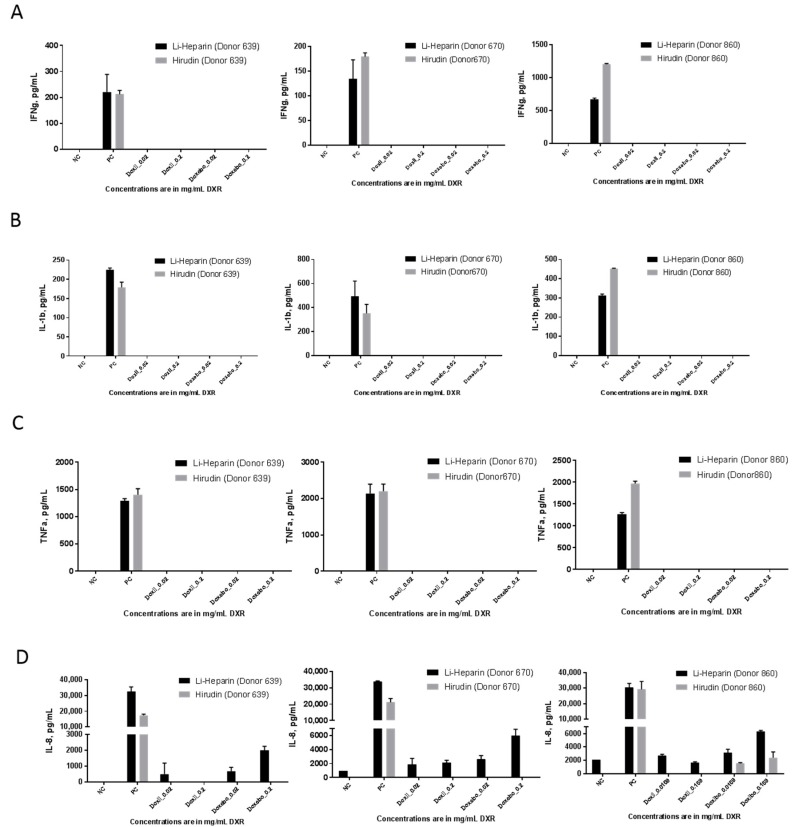
The preclinical safety assessment of novel nanotechnology-based drug products frequently relies on in vitro assays, especially during the early stages of product development, due to the limited quantities of nanomaterials available for such studies. The majority of immunological tests require donor blood. To enable such tests one has to prevent the blood from coagulating, which is usually achieved by the addition of an anticoagulant into blood collection tubes. Heparin, ethylene diamine tetraacetic acid (EDTA), and citrate are the most commonly used anticoagulants. Novel anticoagulants such as hirudin are also available but are not broadly used. Despite the notion that certain anticoagulants may influence assay performance, a systematic comparison between traditional and novel anticoagulants in the in vitro assays intended for immunological characterization of nanotechnology-based formulations is currently not available. We compared hirudin-anticoagulated blood with its traditional counterparts in the standardized immunological assay cascade, and found that the type of anticoagulant did not influence the performance of the hemolysis assay. However, hirudin was more optimal for the complement activation and leukocyte proliferation assays, while traditional anticoagulants citrate and heparin were more appropriate for the coagulation and cytokine secretion assays. The results also suggest that traditional immunological controls such as lipopolysaccharide (LPS ) are not reliable for understanding the role of anticoagulant in the assay performance. We observed differences in the test results between hirudin and traditional anticoagulant-prepared blood for nanomaterials at the time when no such effects were seen with traditional controls. It is, therefore, important to recognize the advantages and limitations of each anticoagulant and consider individual nanoparticles on a case-by-case basis.
Keywords: complement activation; cytokines; hemolysis; immunotoxicity; in vitro; leukocyte proliferation; liposomes; nanoparticles; plasma coagulation; platelet aggregation; safety.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
