

Respiratory muscle training for multiple sclerosis
- PMID: 29267988
- PMCID: PMC6486138
- DOI: 10.1002/14651858.CD009424.pub2
Respiratory muscle training for multiple sclerosis
Abstract
Background: Multiple sclerosis (MS) is a chronic disease of the central nervous system, affecting approximately 2.5 million people worldwide. People with MS may experience limitations in muscular strength and endurance - including the respiratory muscles, affecting functional performance and exercise capacity. Respiratory muscle weakness can also lead to diminished performance on coughing, which may result in (aspiration) pneumonia or even acute ventilatory failure, complications that frequently cause death in MS. Training of the respiratory muscles might improve respiratory function and cough efficacy.
Objectives: To assess the effects of respiratory muscle training versus any other type of training or no training for respiratory muscle function, pulmonary function and clinical outcomes in people with MS.
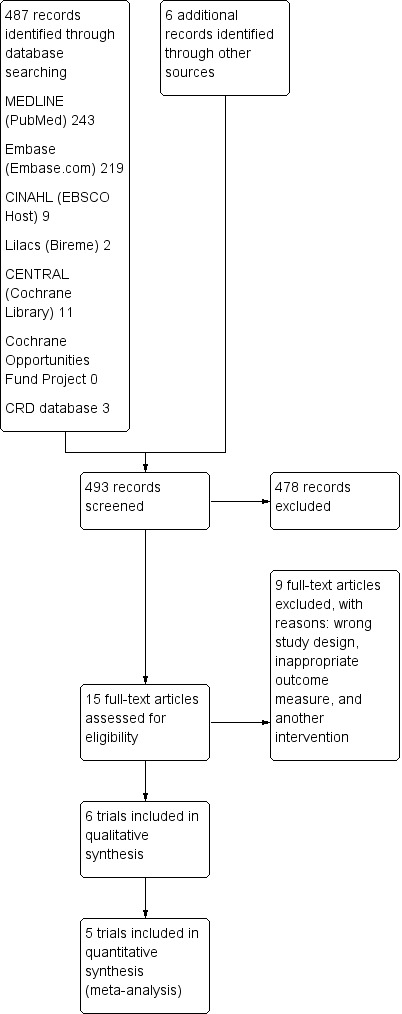
Search methods: We searched the Trials Register of the Cochrane Multiple Sclerosis and Rare Diseases of the Central Nervous System Group (3 February 2017), which contains trials from the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, Embase, CINAHL, LILACS and the trial registry databases ClinicalTrials.gov and WHO International Clinical Trials Registry Platform. Two authors independently screened records yielded by the search, handsearched reference lists of review articles and primary studies, checked trial registers for protocols, and contacted experts in the field to identify further published or unpublished trials.
Selection criteria: We included randomized controlled trials (RCTs) that investigated the efficacy of respiratory muscle training versus any control in people with MS.
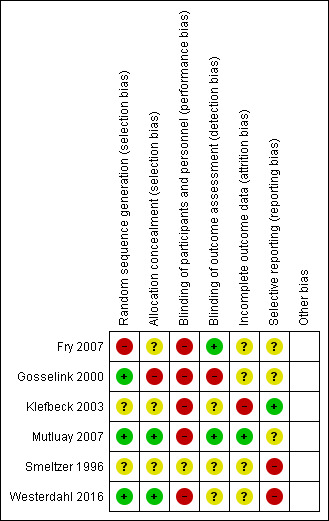
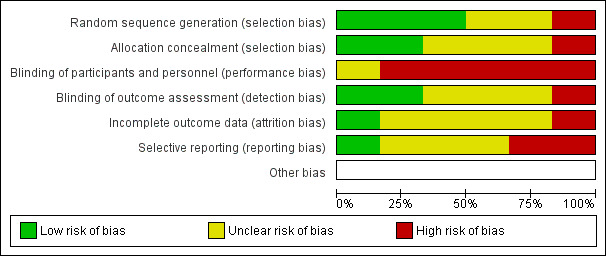
Data collection and analysis: One reviewer extracted study characteristics and study data from included RCTs, and two other reviewers independently cross-checked all extracted data. Two review authors independently assessed risk of bias with the Cochrane 'Risk of bias' assessment tool. When at least two RCTs provided data for the same type of outcome, we performed meta-analyses. We assessed the certainty of the evidence according to the GRADE approach.
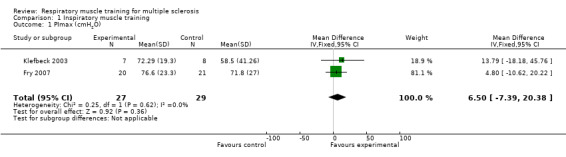
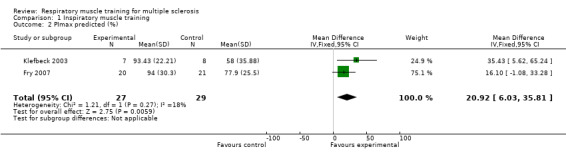
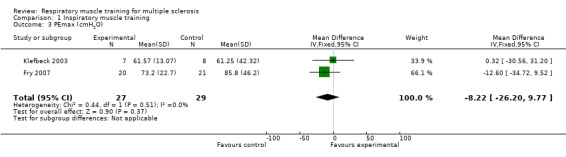
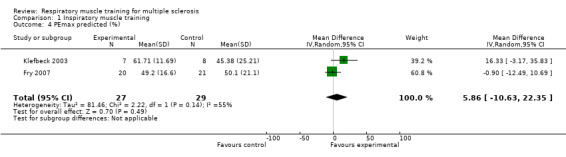
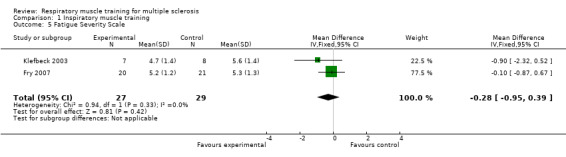
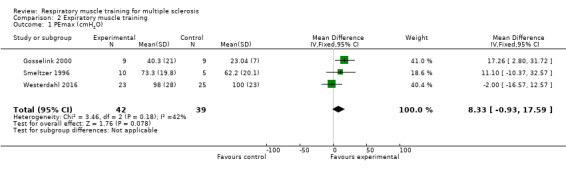
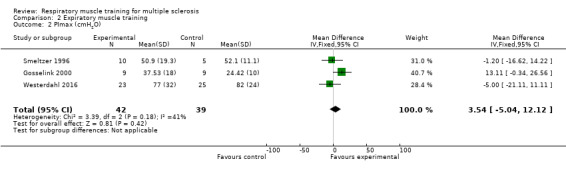
Main results: We included six RCTs, comprising 195 participants with MS. Two RCTs investigated inspiratory muscle training with a threshold device; three RCTs, expiratory muscle training with a threshold device; and one RCT, regular breathing exercises. Eighteen participants (˜ 10%) dropped out; trials reported no serious adverse events.We pooled and analyzed data of 5 trials (N=137) for both inspiratory and expiratory muscle training, using a fixed-effect model for all but one outcome. Compared to no active control, meta-analysis showed that inspiratory muscle training resulted in no significant difference in maximal inspiratory pressure (mean difference (MD) 6.50 cmH2O, 95% confidence interval (CI) -7.39 to 20.38, P = 0.36, I2 = 0%) or maximal expiratory pressure (MD -8.22 cmH2O, 95% CI -26.20 to 9.77, P = 0.37, I2 = 0%), but there was a significant benefit on the predicted maximal inspiratory pressure (MD 20.92 cmH2O, 95% CI 6.03 to 35.81, P = 0.006, I2 = 18%). Meta-analysis with a random-effects model failed to show a significant difference in predicted maximal expiratory pressure (MD 5.86 cmH2O, 95% CI -10.63 to 22.35, P = 0.49, I2 = 55%). These studies did not report outcomes for health-related quality of life.Three RCTS compared expiratory muscle training versus no active control or sham training. Under a fixed-effect model, meta-analysis failed to show a significant difference between groups with regard to maximal expiratory pressure (MD 8.33 cmH2O, 95% CI -0.93 to 17.59, P = 0.18, I2 = 42%) or maximal inspiratory pressure (MD 3.54 cmH2O, 95% CI -5.04 to 12.12, P = 0.42, I2 = 41%). One trial assessed quality of life, finding no differences between groups.For all predetermined secondary outcomes, such as forced expiratory volume, forced vital capacity and peak flow pooling was not possible. However, two trials on inspiratory muscle training assessed fatigue using the Fatigue Severity Scale (range of scores 0-56 ), finding no difference between groups (MD, -0.28 points, 95% CI-0.95 to 0.39, P = 0.42, I2 = 0%). Due to the low number of studies included, we could not perform cumulative meta-analysis or subgroup analyses. It was not possible to perform a meta-analysis for adverse events, no serious adverse were mentioned in any of the included trials.The quality of evidence was low for all outcomes because of limitations in design and implementation as well as imprecision of results.
Authors' conclusions: This review provides low-quality evidence that resistive inspiratory muscle training with a resistive threshold device is moderately effective postintervention for improving predicted maximal inspiratory pressure in people with mild to moderate MS, whereas expiratory muscle training showed no significant effects. The sustainability of the favourable effect of inspiratory muscle training is unclear, as is the impact of the observed effects on quality of life.
Conflict of interest statement
M Rietberg: none known.
J Veerbeek: none known.
R Gosselink: none known.
G Kwakkel: none known.
E van Wegen: none known.
Figures
Update of
References
References to studies included in this review
Fry 2007 {published data only}
-
- Fry DK, Pfalzer LA, Chokshi AR, Wagner MT, Jackson ES. Randomized control trial of effects of a 10‐week inspiratory muscle training program on measures of pulmonary function in persons with multiple sclerosis. Journal of Neurological Physical Therapy 2007;31(4):162‐72. - PubMed
Gosselink 2000 {published data only}
-
- Gosselink R, Kovacs L, Ketelaer P, Carton H, Decramer M. Respiratory muscle weakness and respiratory muscle training in severely disabled multiple sclerosis patients. Archives of Physical Medicine and Rehabilitation 2000;81(6):747‐51. - PubMed
Klefbeck 2003 {published data only}
-
- Klefbeck B, Hamrah Nedjad J. Effect of inspiratory muscle training in patients with multiple sclerosis. Archives of Physical Medicine and Rehabilitation 2003;84(7):994‐9. - PubMed
Mutluay 2007 {published data only}
-
- Mutluay FK, Demir R, Ozyilmaz S, Caglar AT, Altintas A, Gurses HN. Breathing‐enhanced upper extremity exercises for patients with multiple sclerosis. Clinical Rehabilitation 2007;21(7):595‐602. - PubMed
Smeltzer 1996 {published data only}
-
- Smeltzer SC, Lavietes MH, Cook SD. Expiratory training in multiple sclerosis. Archives of Physical Medicine and Rehabilitation 1996;77(9):909‐12. - PubMed
Westerdahl 2016 {published data only}
-
- Westerdahl E, Wittrin A, Kånåhols M, Gunnarsson M, Nilsagård Y. Deep breathing exercises with positive expiratory pressure in patients with multiple sclerosis ‐ a randomized controlled trial. Clinical Respiratory Journal 2016;10(6):698‐706. - PubMed
References to studies excluded from this review
Chiara 2006 {published data only}
-
- Chiara T, Martin AD, Davenport PW, Bolser DC. Expiratory muscle strength training in persons with multiple sclerosis having mild to moderate disability: effect on maximal expiratory pressure, pulmonary function, and maximal voluntary cough. Archives of Physiocal Medicine and Rehabilitation 2006;87(4):468‐73. - PMC - PubMed
Chiara 2007 {published data only}
-
- Chiara T, Martin D, Sapienza C. Expiratory muscle strength training: speech production outcomes in patients with multiple sclerosis. Neurorehabilitation and Neural Repair 2007;21(3):239‐49. - PubMed
Feltman 2013 {published data only}
-
- Feltham MG, Collett J, Izadi H, Wade DT, Morris MG, Meaney AJ, et al. Cardiovascular adaptation in people with multiple sclerosis following a twelve week exercise programme suggest deconditioning rather than autonomic dysfunction caused by the disease results from a randomized controlled trial. European Journal of Physical Rehabilitation Medicine 2013;49(6):765‐74. - PubMed
Hansen 2015 {published data only}
-
- Hansen D, Wens I, Keytsman C, Verboven K, Dendale P, Eijnde BO. Ventilatory function during exercise in multiple sclerosis and impact of training intervention: cross‐sectional and randomized controlled trial. European Journal of Physical Rehabilitation Medicine 2015;51(5):557‐68. - PubMed
Natour 2012 {published data only}
-
- Natour Y, Marie B, Aljunidy L. The respiratory muscle capabilities of Jordanian patients with multiple sclerosis. Journal of Voice 2012;26(6):e15‐18. - PubMed
Olgiati 1989 {published data only}
-
- Olgiati R, Girr A, Hügi L, Haegi V. Respiratory muscle training in multiple sclerosis: a pilot study. Schweizer Archiv für Neurologie und Psychiatrie 1989;140(1):46‐50. - PubMed
Pfalzer 2011 {published data only}
Rampello 2007 {published data only}
-
- Rampello A, Franceschini M, Piepoli M, Antenucci R, Lenti G, Olivieri D, et al. Effect of aerobic training on walking capacity and maximal exercise tolerance in patients with multiple sclerosis: a randomized crossover controlled study. Physical Therapy 2007;87(5):545‐55. - PubMed
Ray 2013 {published data only}
-
- Ray AD, Udhoji S, Mashtare TL, Fisher NM. A combined inspiratory and expiratory muscle training program improves respiratory muscle strength and fatigue in multiple sclerosis. Archives of Physical Medicine and Rehabilitation 2013;94(10):1964‐70. - PubMed
References to ongoing studies
NCT00856518 {unpublished data only}
-
- NCT00856518. Expiratory muscle training for persons with neurodegenerative disease [Expiratory muscle training for persons with neurodegenerative disease]. clinicaltrials.gov/ct2/show/record/NCT00856518?term=NCT00856518&rank=1 (first received 3 March 2009).
NCT02104492 {unpublished data only}
-
- NCT02104492. Effects of a 12‐week respiratory muscles training program in persons with relapsing‐ remitting multiple sclerosis [Clinical research on the effect of a 12‐week respiratory muscles training program in persons with relapsing‐remitting multiple sclerosis]. clinicaltrials.gov/ct2/show/record/NCT02104492?term=NCT02104492&rank=1 (first received 27 March 2014).
NCT02726672 {unpublished data only}
-
- NCT02726672. Fatigue and inspiratory muscles training in patients with multiple sclerosis [Fatigue and inspiratory muscles training against resistance in patients with multiple sclerosis with severe disabilities]. clinicaltrials.gov/ct2/show/record/NCT02726672?term=NCT02726672&rank=1 (first received 22 March 2016).
Additional references
Berlowitz 2013
Bosnak‐Guclu 2012
-
- Bosnak‐Guclu M, Gunduz AG, Nazliel B, Irkec C. Comparison of functional exercise capacity, pulmonary function and respiratory muscle strength in patients with multiple sclerosis with different disability levels and healthy controls. Journal of Rehabilitation Medicine 2012;44(1):80‐6. - PubMed
EuroQol 1990
-
- EuroQol Group. EuroQol: a new facility for the measurement of health‐related quality of life. HealthPolicy (New York) 1990;16(3):199–208. - PubMed
Ferreira 2016
-
- Ferreira G, Costa A, Plentz R, Coronel C, Sbruzzi G. Respiratory training improved ventilatory function and respiratory muscle strength in patients with multiple sclerosis and lateral amyotrophic sclerosis: systematic review and meta‐analysis. Physiotherapy 2016;102(3):221‐8. - PubMed
Foglio 1994
-
- Foglio K, Clini E, Facchetti D, Vitacca M, Marangoni S, Bonomelli M, et al. Respiratory muscle function and exercise capacity in multiple sclerosis. European Respiratory Journal 1994;7(1):23‐8. - PubMed
Gomes‐Neto 2016
-
- Gomes‐Neto M, Saquetto MB, Silva CM, Carvalho VO, Ribeiro N, Conceição CS. Effects of respiratory muscle training on respiratory function, respiratory muscle strength, and exercise tolerance in patients post stroke: a systematic review with meta‐analysis. Archives of Physical Medicine and Rehabilitation 2016;97(11):1994‐2001. - PubMed
Higgins 2011
-
- Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of InterventionsVersion 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Koch‐Henriksen 2010
-
- Koch‐Henriksen N, Sørensen PS. The changing demographic pattern of multiple sclerosis epidemiology. Lancet Neurology 2010;9(5):520‐32. - PubMed
Laciuga 2014
-
- Laciuga H, Rosenbek JC, Davenport PW, Sapienza CM. Functional outcomes associated with expiratory muscle strength training: narrative review. Journal of Rehabilitation Research & Development 2014;51(4):535‐46. - PubMed
Martín‐Valero 2014
-
- Martín‐Valero R, Zamora‐Pascual N, Armenta‐Peinado JA. Training of respiratory muscles in patients with multiple sclerosis: a systematic review. Respiratory Care 2014;59(11):1764‐72. - PubMed
McDonald 2001
-
- McDonald WI, Compston A, Edan G, Goodkin D, Hartung HP, Lublin FD, et al. Recommended diagnostic criteria for multiple sclerosis: guidelines from the International Panel on the diagnosis of multiple sclerosis. Annals of Neurology 2001;50(1):121‐7. - PubMed
Motl 2011a
Motl 2011b
-
- Motl RW, McAuley E, Wynn D, Suh Y, Weikert M. Effects of change in fatigue and depression on physical activity over time in relapsing‐remitting multiple sclerosis. Psychology, Health & Medicine 2011;16(1):1‐11. - PubMed
Neder 1999
-
- Neder JA, Andreoni S, Lerario MC, Nery LE. Reference values for lung function tests. II. maximal respiratory pressures and voluntary ventilation. Brazilian Journal of Medical and Biological Research 1999;32(6):719‐27. - PubMed
Polman 2005
-
- Polman CH, Reingold SC, Edan G, Filippi M, Hartung HP, Kappos L, et al. Diagnostic criteria for multiple sclerosis: 2005 revisions to the "McDonald Criteria". Annals of Neurology 2005;58(6):840‐6. - PubMed
Poser 1983
-
- Poser C, Paty D, Scheinberg L. New diagnostic criteria for multiple sclerosis: guidelines for research protocols. Annals of Neurology 1983;13(3):227‐31. - PubMed
RevMan 2014 [Computer program]
-
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Reyes 2013
-
- Reyes A, Ziman M, Nosaka K. Respiratory muscle training for respiratory deficits in neurodegenerative disorders: a systematic review. Chest 2013;143(5):1386‐94. - PubMed
Rietberg 2010
-
- Rietberg MB, Wegen EEH, Kwakkel G. Measuring fatigue in patients with multiple sclerosis: reproducibility, responsiveness and concurrent validity of three Dutch self‐report questionnaires. Disability and Rehabilitation 2010;32(22):1870–6. - PubMed
Rietberg 2016a
-
- Rietberg, MB. [Request for additional results [personal communication]]. Email to: R.Gosselink 11‐02‐2016.
Rietberg 2016b
-
- Rietberg, MB. [Request for additional results [personal communication]]. Email to: B. Klefbeck 11‐02‐2016.
Rietberg 2016c
-
- Rietberg, MB. [Request for additional results [personal communication]]. Email to: SC Smeltzer 11‐02‐2016.
Schumacher 1965
-
- Schumacher GA, Beebe GW, Kibler RF, Kurland LT, Kurtzke JF, McDowell F, et al. Problems of experimental trials of therapy in multiple sclerosis. Annals of the New York Academy of Science 1965;31(122):552‐68. - PubMed
Smeltzer 1988
-
- Smeltzer SC, Utell MJ, Rudick RA, Herndon RM. Pulmonary function and dysfunction in multiple sclerosis. Archives of Neurology 1988;45(11):1245‐9. - PubMed
Smith Hammond 2001
-
- Smith Hammond CA, Goldstein LB, Zajac DJ, Gray L, Davenport PW, Bolser DC. Assessment of aspiration risk in stroke patients with quantification of voluntary cough. Neurology 2001;56(4):502‐6. - PubMed
Stuke 2009
-
- Stuke K, Flachenecker P, Zettl UK, Elias WG, Freidel M, Haas J, et al. Symptomatology of MS: results from the German MS Registry. Journal of Neurology 2009;256(11):1932‐5. - PubMed
Sumelahti 2010
-
- Sumelahti ML, Hakama M, Elovaara I, Pukkala E. Causes of death among patients with multiple sclerosis. Multiple Sclerosis 2010;16(12):1437‐42. - PubMed
Toomey 2012
-
- Toomey E, Coote SB. Physical rehabilitation interventions in nonambulatory people with multiple sclerosis: a systematic review. International Journal of Rehabilitation Research 2012;35(4):281‐91. - PubMed
WHO 2001
-
- World Health Organization. International Classification of Function, Disability and Health. Geneva: World Health Organization, 2001.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical