

Replacement of calcified ascending aorta in patients undergoing aortic valve replacement
- PMID: 29268511
- PMCID: PMC5721034
- DOI: 10.21037/jtd.2017.10.100
Replacement of calcified ascending aorta in patients undergoing aortic valve replacement
Abstract
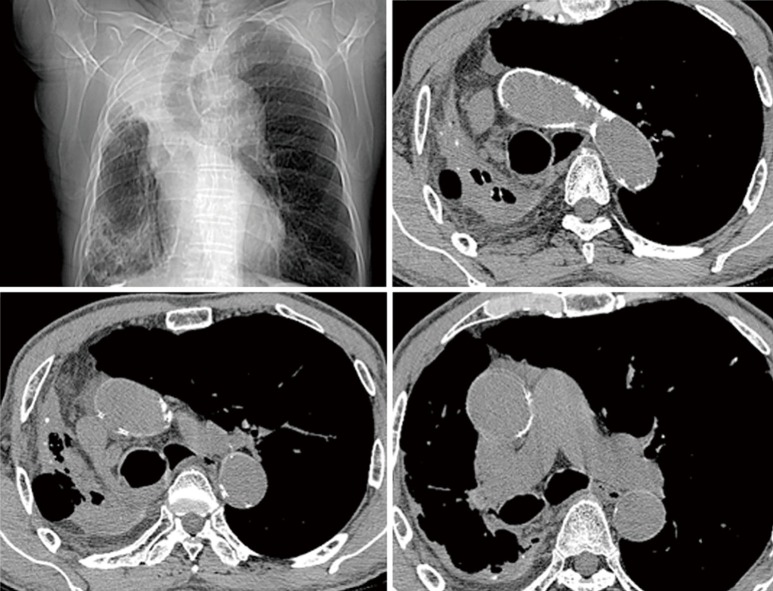
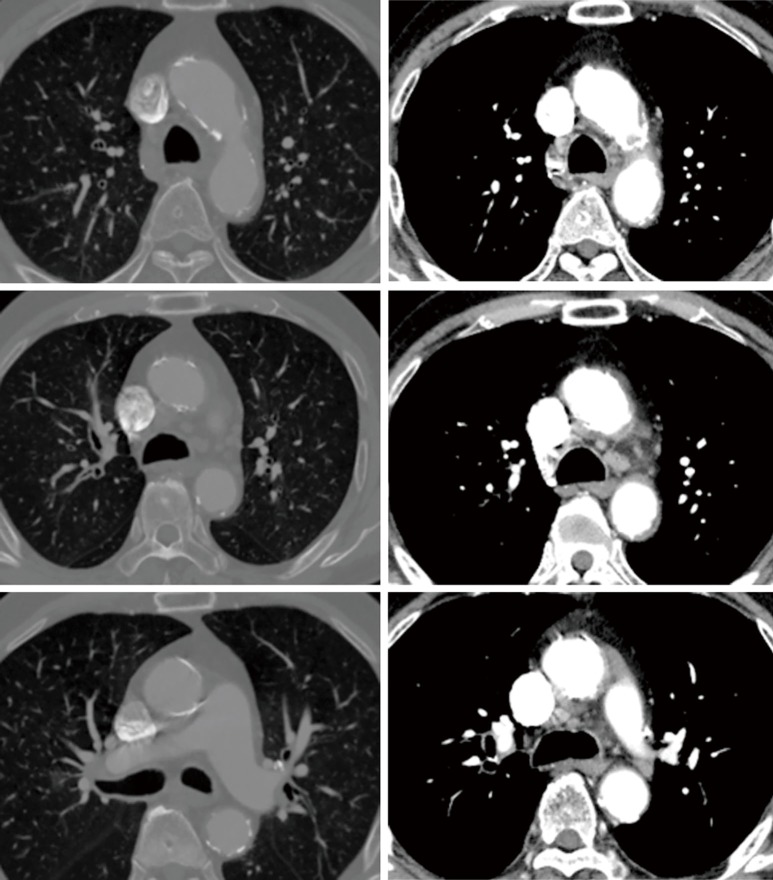
Background: Aortic stenosis (AS) with an extensively calcified ascending aorta is a growing indication for transcatheter aortic valve implantation (TAVI) because aortic manipulation during surgical aortic valve replacement (AVR) is unsafe in these patients. The aim of this study was to evaluate the outcomes of AVR plus ascending aorta replacement (AAR) in patients with severe AS and a heavily calcified ascending aorta.
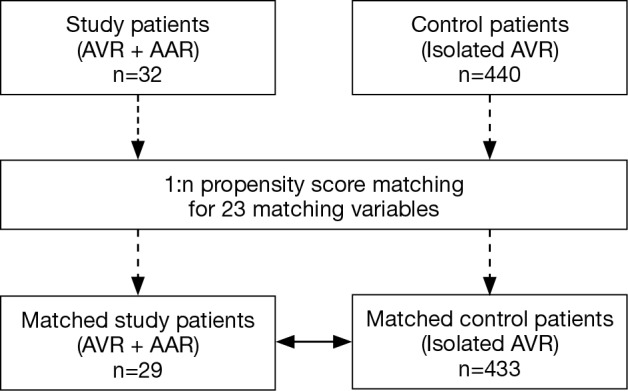
Methods: From 2004 to 2014, a total of 32 patients with severe AS and extensive aortic calcification underwent concomitant first-time AVR and AAR (AVR + AAR). The mean patient age was 74±7 (range, 59-87) years, and 7 (22%) patients were octogenarians. The mean logistic EuroSCORE was 21.4%±19.0% (range, 3.3-68.2%). Arterial cannulae were placed at the ascending aorta (n=26, 81%), aortic arch (n=5, 16%), or axillary artery (n=1, 3%). The aorta was not clamped, and circulatory arrest was used in all patients. One-to-many (1:n) propensity score matching between the study population (AVR + AAR, n=29) and control group (isolated AVR for severe AS, n=433) was performed.
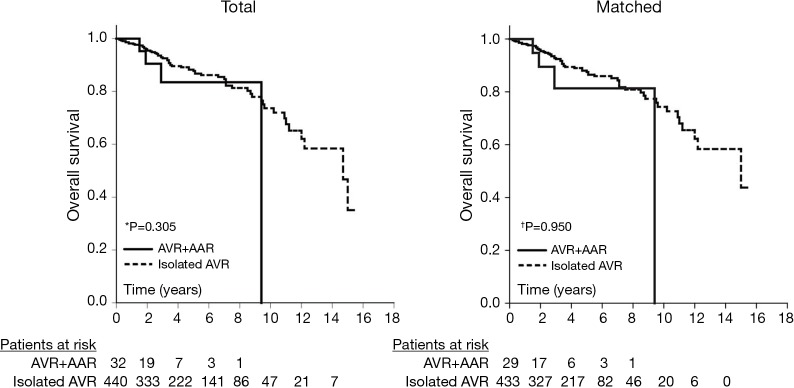
Results: There was no early mortality in the study population. Postoperative neurologic complications included a minor stroke, which resolved without sequelae at discharge, and a transient ischemic attack. The 5-year survival rate was 83%±9%. In the propensity score-matched comparison, 5-year survival was not significantly different between groups; 81%±10% in the AVR + AAR group vs. 87%±2% in the isolated AVR group (P=0.950).
Conclusions: Surgical AVR with AAR in AS patients with calcified ascending aortas led to acceptable early and late outcomes. Although the applications for TAVI are growing, a surgical approach may be an alternative option for relatively younger patients with severely calcified aorta.
Keywords: Aortic valve stenosis; deep hypothermic circulatory arrest (DHCA); thoracic aorta; vascular calcification.
Conflict of interest statement
Conflicts of Interest: Part of this research was presented at the 29th Annual Meeting of the European Association of Cardiothoracic Surgeons, Amsterdam, Netherlands, October 3-7, 2015.
Figures
Similar articles
-
The safety of deep hypothermic circulatory arrest in aortic valve replacement with unclampable aorta in non-octogenarians.Interact Cardiovasc Thorac Surg. 2015 Jan;20(1):79-84. doi: 10.1093/icvts/ivu314. Epub 2014 Sep 21. Interact Cardiovasc Thorac Surg. 2015. PMID: 25246009
-
[Aortic Valve Surgery for Patients with Severely Calcified Aorta].Kyobu Geka. 2020 Sep;73(10):744-748. Kyobu Geka. 2020. PMID: 33130759 Japanese.
-
Impact of concomitant replacement of the ascending aorta in patients undergoing aortic valve replacement on operative morbidity and mortality.Eur J Cardiothorac Surg. 2022 Feb 18;61(3):587-593. doi: 10.1093/ejcts/ezab420. Eur J Cardiothorac Surg. 2022. PMID: 34626175
-
[Aortic valve surgery for patients with severely calcified aorta].Kyobu Geka. 2012 Jul;65(8):648-52. Kyobu Geka. 2012. PMID: 22868422 Japanese.
-
[Percutaneous aortic valve implantation - contra].Herz. 2009 Mar;34(2):130-9. doi: 10.1007/s00059-009-3201-1. Herz. 2009. PMID: 19370329 Review. German.
References
-
- Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014;63:e57-185. 10.1016/j.jacc.2014.02.536 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials