

Clinical consensus of emergency airway management
- PMID: 29268532
- PMCID: PMC5721045
- DOI: 10.21037/jtd.2017.10.79
Clinical consensus of emergency airway management
Abstract
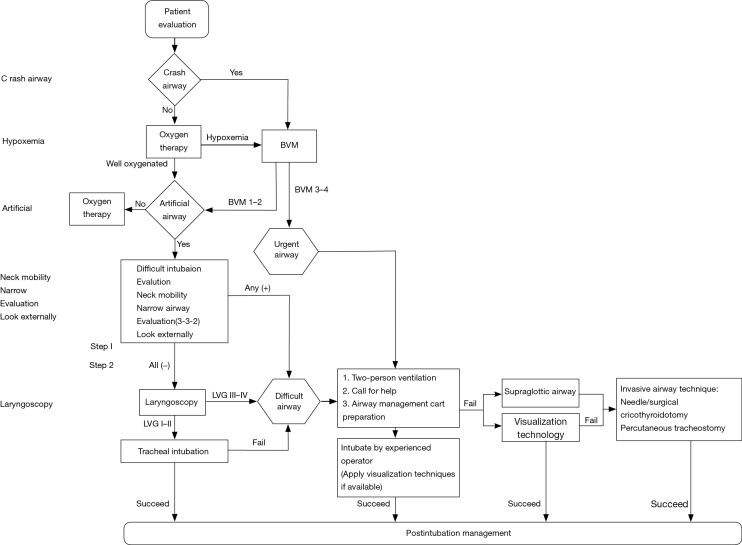
Airway management is a common and key method to maintain and improve external respiration function of patients. Emergency physicians need a more appropriate guide to airway management. We concisely concluded current circumstances of Chinese emergency airway management. Then, we raised four principles: (I) priority to ventilation and oxygenation; (II) evaluation before intubation; (III) higher level of preparation (de-escalation); (IV) simplest (and least potentially harmful) form of intubation. We raised "CHANNEL" flow to direct initial emergency airway management and an algorithm was showed for emergency physicians understanding key points of airway management and further making medical decision. Finally, we introduced pharmacology of airway management.
Keywords: Emergency medicine; airway management; intubation; tracheostomy.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures

References
-
- Yu BW, Wu XM, Zuo MZ, et al. Difficult Airway Management Guidelines. J Clini Anesth 2013;29:93-8.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources