

Infectious pleural effusion status and treatment progress
- PMID: 29268539
- PMCID: PMC5720994
- DOI: 10.21037/jtd.2017.10.96
Infectious pleural effusion status and treatment progress
Abstract
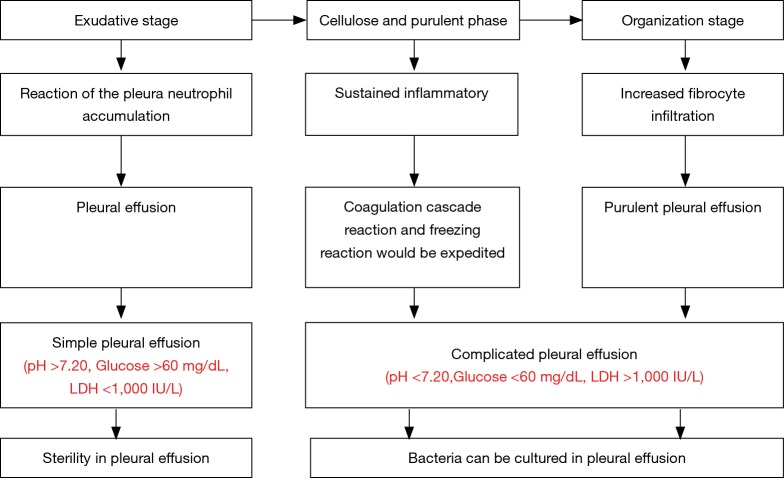
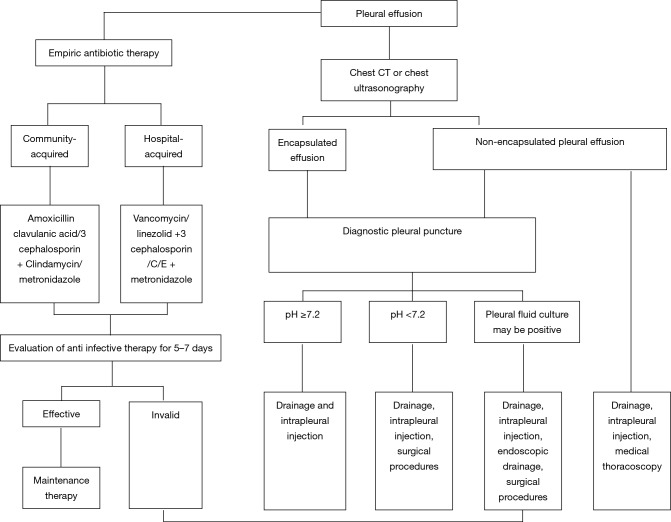
Pleural cavity infection continuously seriously threatens human health with continuous medical progress. From the perspective of pathophysiology, it can be divided into three stages: exudative stage, fibrin exudation and pus formation stage, and organization stage. Due to the pathogenic bacteria difference of pleural cavity infection and pulmonary infection, it is very important for disease treatment to analyze the bacteria and biochemical characteristics of the infectious pleural effusion. Most prognoses of patients have been relatively good, while for some patients, the complicated parapneumonic effusion or empyema could be evolved. Antibiotic treatment and sufficient drainage are the foundation for this treatment. No evidence can support the routine use of a fibrin agent. However, it has been reported that the plasminogen activator and deoxyribonuclease can be recommended to be applied in the pleural cavity. In case of failure on conservative medical treatment, operative treatment can be applied such as thoracoscopy and pleural decortication. According to the clinical characteristics of these patients, it is a key to research prognosis, as well as early evaluation and stratification, in the future.
Keywords: Infectious pleural effusion; empyema; status quo; treatment progress.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources