

Falls efficacy, postural balance, and risk for falls in older adults with falls-related emergency department visits: prospective cohort study
- PMID: 29268720
- PMCID: PMC5740922
- DOI: 10.1186/s12877-017-0682-2
Falls efficacy, postural balance, and risk for falls in older adults with falls-related emergency department visits: prospective cohort study
Abstract
Background: Risk for falls in older adults has been associated with falls efficacy (self-perceived confidence in performing daily physical activities) and postural balance, but available evidence is limited and mixed. We examined the interaction between falls efficacy and postural balance and its association with future falls. We also investigated the association between falls efficacy and gait decline.
Methods: Falls efficacy, measured by the Modified Falls Efficacy Scale (MFES), and standing postural balance, measured using computerized posturography on a balance board, were obtained from 247 older adults with a falls-related emergency department visit. Six-month prospective fall rate and habitual gait speed at 6 months post baseline assessment were also measured.
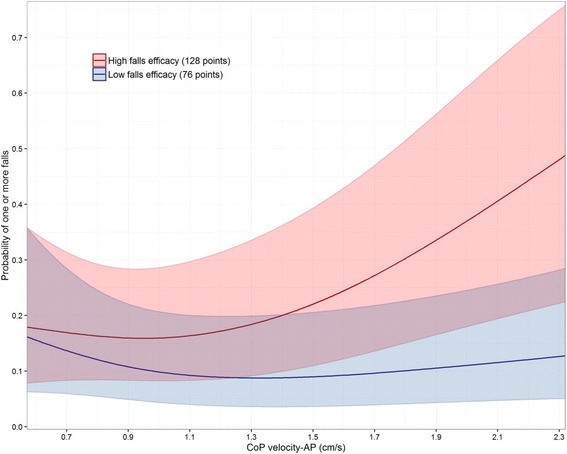
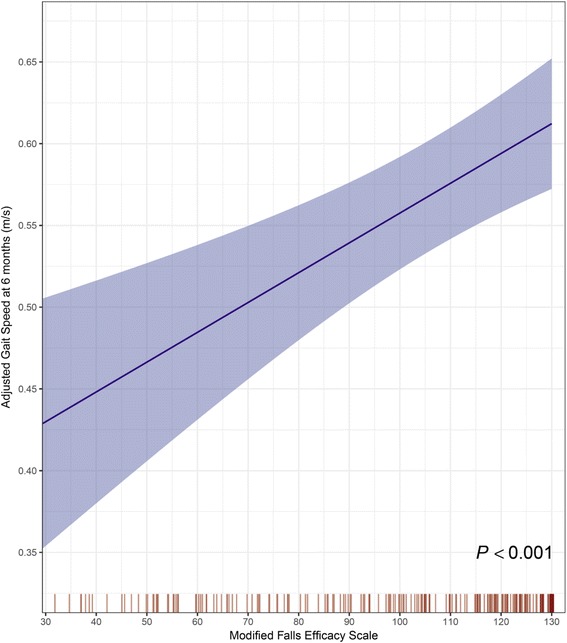
Results: In multivariable proportional odds analyses adjusted for potential confounders, falls efficacy modified the association between postural balance and fall risk (interaction P = 0.014): increasing falls efficacy accentuated the increased fall risk related to poor postural balance. Low baseline falls efficacy was strongly predictive of worse gait speed (0.11 m/s [0.06 to 0.16] slower gait speed per IQR decrease in MFES; P < 0.001).
Conclusion: Older adults with high falls efficacy but poor postural balance were at greater risk for falls than those with low falls efficacy; however, low baseline falls efficacy was strongly associated with worse gait function at follow-up. Further research into these subgroups of older adults is warranted.
Trial registration: ClinicalTrials.gov identifier: NCT01713543 .
Keywords: Balance; Falls; Falls efficacy.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the centralised institutional review board (2012/147/A) and registered on 24 October 2012 with the U.S. Clinical Trial Registry (NCT01713543). All participants provided written informed consent.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Ayoung-Chee P, McIntyre L, Ebel BE, Mack CD, McCormick W, and Maier RV. Long-term outcomes of ground-level falls in the elderly. J Trauma Acute Care Surg 2014; 76: 498–503; discussion 503. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
