

PAR4 (Protease-Activated Receptor 4) Antagonism With BMS-986120 Inhibits Human Ex Vivo Thrombus Formation
- PMID: 29269513
- PMCID: PMC5779320
- DOI: 10.1161/ATVBAHA.117.310104
PAR4 (Protease-Activated Receptor 4) Antagonism With BMS-986120 Inhibits Human Ex Vivo Thrombus Formation
Abstract
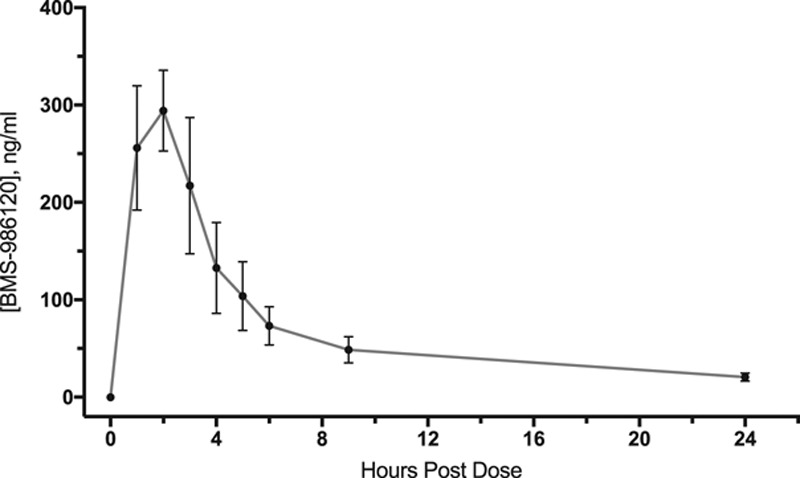
Objective: BMS-986120 is a novel first-in-class oral PAR4 (protease-activated receptor 4) antagonist with potent and selective antiplatelet effects. We sought to determine for the first time, the effect of BMS-986120 on human ex vivo thrombus formation.
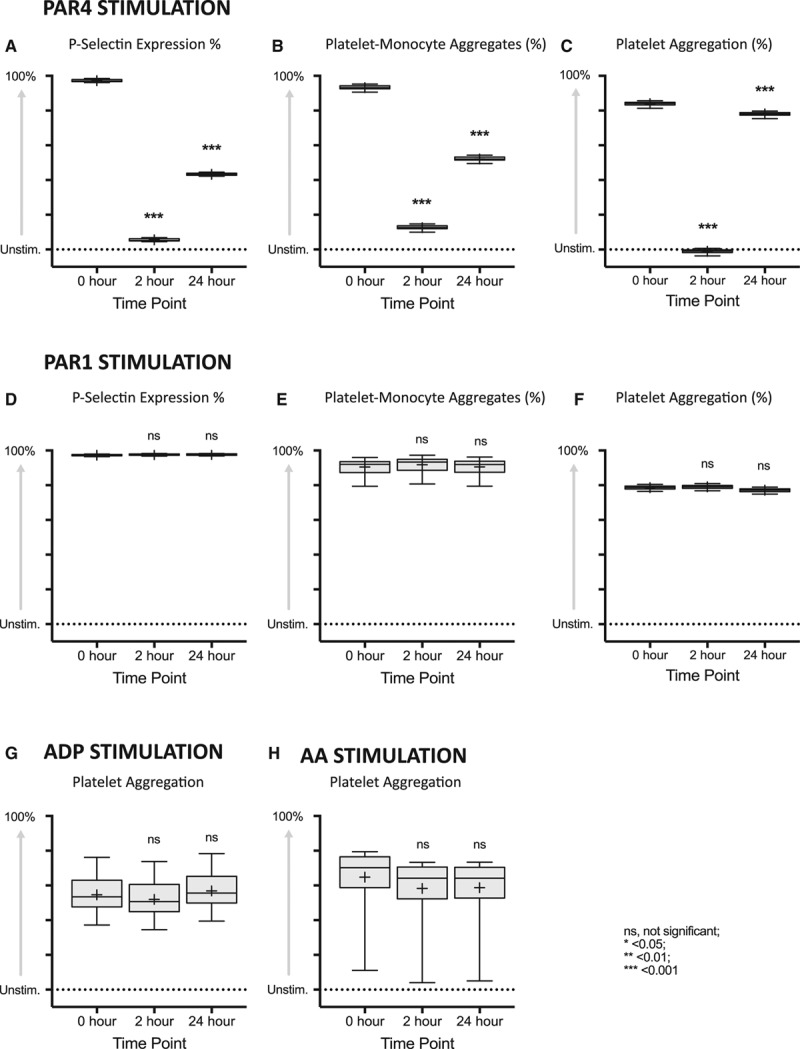
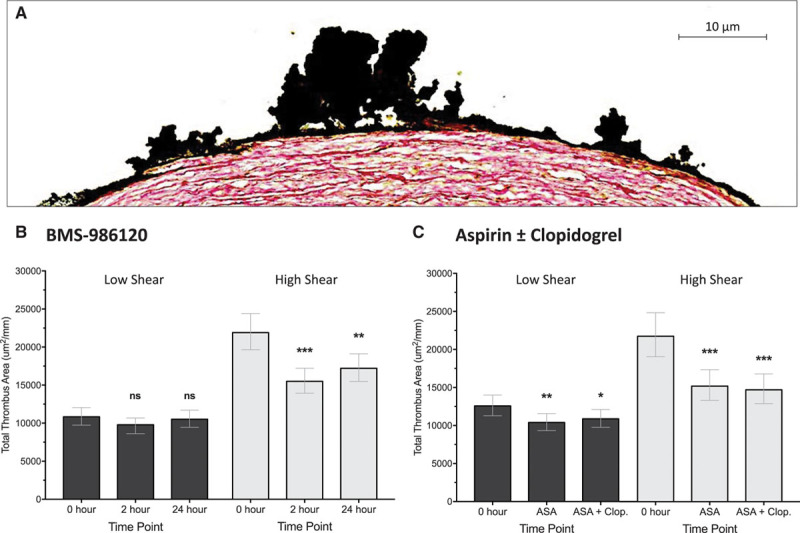
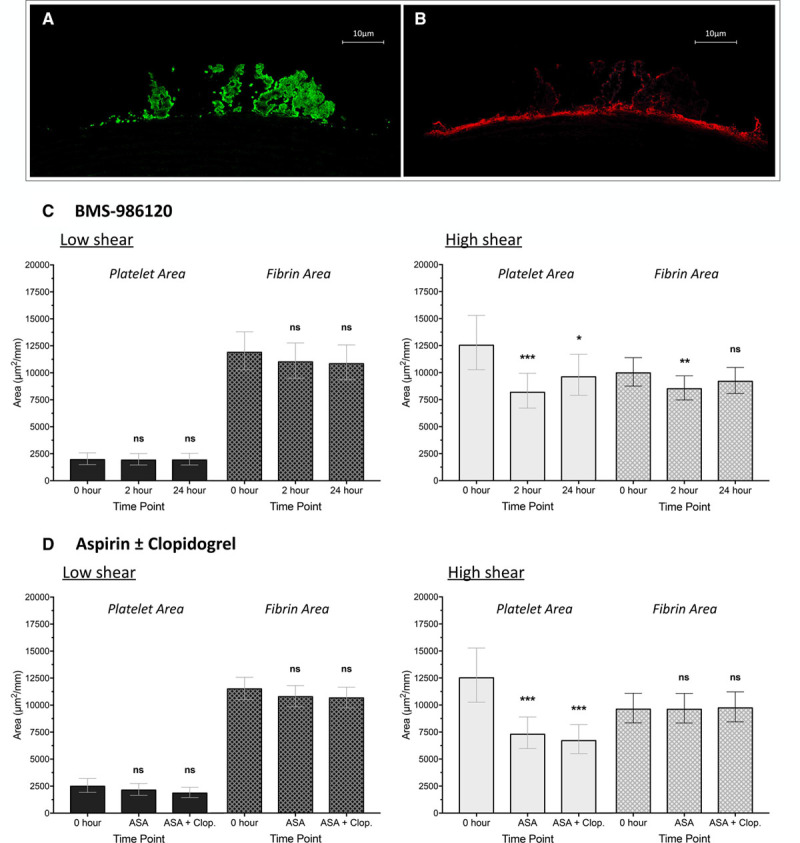
Approach and results: Forty healthy volunteers completed a phase 1 parallel-group PROBE trial (Prospective Randomized Open-Label Blinded End Point). Ex vivo platelet activation, platelet aggregation, and thrombus formation were measured at 0, 2, and 24 hours after (1) oral BMS-986120 (60 mg) or (2) oral aspirin (600 mg) followed at 18 hours with oral aspirin (600 mg) and oral clopidogrel (600 mg). BMS-986120 demonstrated highly selective and reversible inhibition of PAR4 agonist peptide (100 μM)-stimulated P-selectin expression, platelet-monocyte aggregates, and platelet aggregation (P<0.001 for all). Compared with pretreatment, total thrombus area (μm2/mm) at high shear was reduced by 29.2% (95% confidence interval, 18.3%-38.7%; P<0.001) at 2 hours and by 21.4% (9.3%-32.0%; P=0.002) at 24 hours. Reductions in thrombus formation were driven by a decrease in platelet-rich thrombus deposition: 34.8% (19.3%-47.3%; P<0.001) at 2 hours and 23.3% (5.1%-38.0%; P=0.016) at 24 hours. In contrast to aspirin alone, or in combination with clopidogrel, BMS-986120 had no effect on thrombus formation at low shear (P=nonsignificant). BMS-986120 administration was not associated with an increase in coagulation times or serious adverse events.
Conclusions: BMS-986120 is a highly selective and reversible oral PAR4 antagonist that substantially reduces platelet-rich thrombus formation under conditions of high shear stress. Our results suggest PAR4 antagonism has major potential as a therapeutic antiplatelet strategy.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier: NCT02439190.
Keywords: antiplatelet; human; novel; protease-activated receptor 4; thrombosis.
© 2017 The Authors.
Figures
Comment in
-
PAR4 (Protease-Activated Receptor 4): PARticularly Important 4 Antiplatelet Therapy.Arterioscler Thromb Vasc Biol. 2018 Feb;38(2):287-289. doi: 10.1161/ATVBAHA.117.310550. Arterioscler Thromb Vasc Biol. 2018. PMID: 29367229 Free PMC article. No abstract available.
References
-
- Amsterdam EA, Wenger NK, Brindis RG, et al. ACC/AHA Task Force Members. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association task force on practice guidelines. Circulation. 2014;130:e344–e426. doi: 10.1161/CIR.0000000000000134. - PubMed
-
- Steg PG, James SK, Atar D Task Force on the management of ST-segment elevation acute myocardial infarction of the European Society of Cardiology (ESC) ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J. 2012;33:2569–2619. doi: 10.1093/eurheartj/ehs215. - PubMed
-
- Roffi M, Patrono C, Collet JP, et al. Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: task force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur Heart J. 2016;37:267–315. doi: 10.1093/eurheartj/ehv320. - PubMed
-
- Geeganage CM, Diener HC, Algra A, Chen C, Topol EJ, Dengler R, Markus HS, Bath MW, Bath PM Acute Antiplatelet Stroke Trialists Collaboration. Dual or mono antiplatelet therapy for patients with acute ischemic stroke or transient ischemic attack: systematic review and meta-analysis of randomized controlled trials. Stroke. 2012;43:1058–1066. doi: 10.1161/STROKEAHA.111.637686. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
