

Center Variation and the Effect of Center and Provider Characteristics on Clinical Outcomes in Kidney Transplantation: A Systematic Review of the Evidence
- PMID: 29270300
- PMCID: PMC5731624
- DOI: 10.1177/2054358117735523
Center Variation and the Effect of Center and Provider Characteristics on Clinical Outcomes in Kidney Transplantation: A Systematic Review of the Evidence
Abstract
Background: Kidney transplantation is the best treatment option for patients with end-stage renal disease. While patient-level factors affecting survival are established, the presence of variation in the management of transplant recipients remains unknown.
Objective: The objective of this study was to examine center variation in kidney transplantation and identify center and provider characteristics that may be associated with clinical outcomes.
Design: This is a systematic review.
Data sources: Ovid Medline, Embase, and Cochrane library from inception to June 2016 were used.
Study eligibility: Any study examining the association between center or provider characteristics and graft or patient survival, quality of life, or functional status were included.
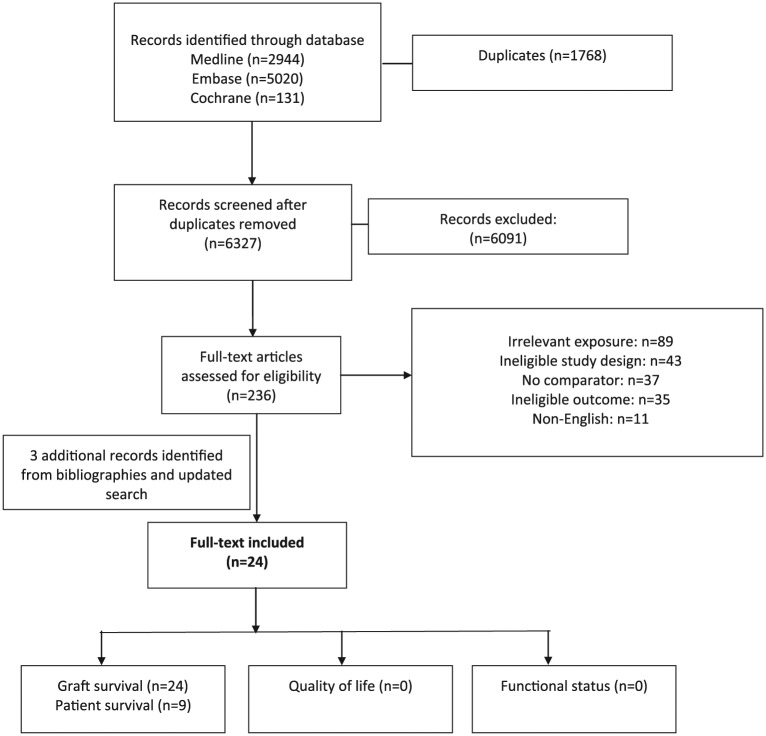
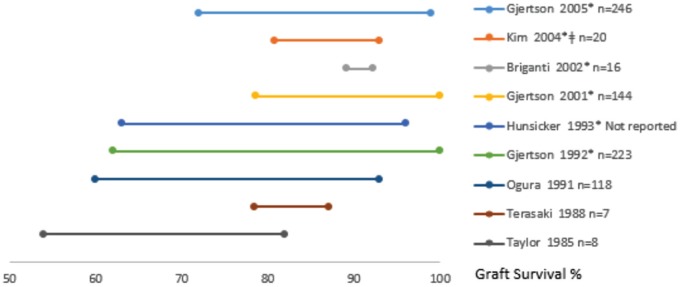
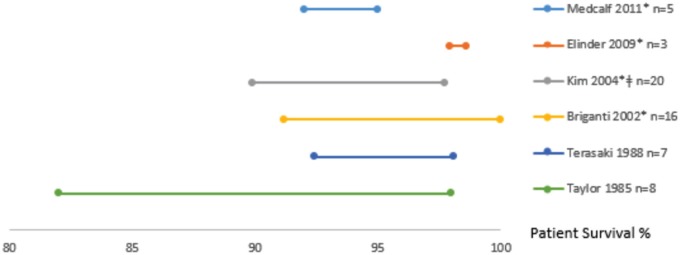
Results: We identified 6327 records and 24 studies met eligibility. Most studies used data registries. Characteristics evaluated include center volume (n = 17), provider volume (n = 2), provider experience (n = 1), center type (n = 2), and location of follow-up (n = 1). Outcomes assessed included graft survival (n = 24) and patient survival (n = 9). Significant center variation was described in 12 of 15 and 5 of 7 studies for graft and patient survival. There was a significant and positive association between center volume and graft and patient survival in 8 and 2 studies, respectively. Provider experience and volume were significantly associated with less allograft loss and provider volume with lower risk of death. There was no association between graft survival and location of follow-up or center type.
Limitations: There was substantial heterogeneity in the variables assessed and methodology used to analyze associations.
Conclusion: This systematic review found center variation in kidney transplantation. Future studies in the current era are necessary to better evaluate this important topic.
Contexte: La transplantation constitue la meilleure option de traitement pour les patients atteints d’insuffisance rénale terminale. Alors que les facteurs relatifs au patient et susceptibles d’affecter sa survie sont bien établis, nous ignorons s’il existe des variations dans la manière dont sont pris en charge les receveurs d’une greffe.
Objectifs de l’étude: Nous voulions observer les différences entre les centres de greffe rénale et cibler les caractéristiques propres à un établissement ou à un fournisseur de soins qui seraient susceptibles d’influencer les résultats cliniques des patients.
Type d’étude: Il s’agit d’une revue systématique.
Sources: Nous avons consulté des études répertoriées dans les bases de données suivantes : Ovid Medline, Embase et la bibliothèque Cochrane, depuis leur création jusqu’en juin 2016.
Admissibilité à l’étude: Ont été retenues toutes les études portant sur une association entre les caractéristiques du centre de greffe rénale ou du fournisseur de soins et la survie du greffon ou du patient, la qualité de vie du patient ou son état fonctionnel.
Résultats: La plupart des études répertoriées avaient utilisé des registres de données. Des 6 327 registres consultés, seuls 24 satisfaisaient les critères d’admissibilité de l’étude. Parmi les caractéristiques évaluées, on compte le volume de patients de l’établissement (n = 17), le volume de patients suivis par le fournisseur de soins (n = 2), l’expérience du fournisseur de soins (n = 1), le type d’établissement (n = 2) et le site du suivi (n = 1). La survie du greffon (n = 24) et la survie du patient (n = 9) constituaient les résultats cliniques évalués. On a affirmé une variation significative entre centres de greffe dans 12 de 15 études quant à la survie du greffon, et dans 5 de 7 études quant à la survie du patient. On a observé une corrélation positive significative entre le volume de patients de l’établissement et la survie du greffon (8 études) et celle du patient (2 études). L’expérience du fournisseur de soins, tout comme le volume de patients pris en charge, a été associée significativement à un taux réduit de perte du greffon. Qui plus est, le volume de patients traités par le fournisseur de soins a aussi été associé à un risque de mortalité amoindri. Par contre, nous n’avons pu établir de corrélation entre le site du suivi ou le type d’établissement et la probabilité de survie du greffon.
Limites de l’étude: On a noté une forte hétérogénéité dans les études consultées en ce qui concerne les variables évaluées et la méthodologie utilisée pour établir les corrélations.
Conclusion: Notre revue systématique a permis de constater une grande variabilité entre établissements en regard de la transplantation rénale. Des études ultérieures, basées sur des données plus récentes, seraient nécessaires pour une évaluation plus précise de cet enjeu substantiel.
Keywords: allograft survival; center variation; kidney transplantation; quality of life.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
Association of Kidney Transplant Center Volume With 3-Year Clinical Outcomes.Am J Kidney Dis. 2019 Oct;74(4):441-451. doi: 10.1053/j.ajkd.2019.02.019. Epub 2019 May 7. Am J Kidney Dis. 2019. PMID: 31076173 Free PMC article.
-
Kidney and liver organ transplantation in persons with human immunodeficiency virus: An Evidence-Based Analysis.Ont Health Technol Assess Ser. 2010;10(4):1-56. Epub 2010 Mar 1. Ont Health Technol Assess Ser. 2010. PMID: 23074407 Free PMC article.
-
Beyond the black stump: rapid reviews of health research issues affecting regional, rural and remote Australia.Med J Aust. 2020 Dec;213 Suppl 11:S3-S32.e1. doi: 10.5694/mja2.50881. Med J Aust. 2020. PMID: 33314144
-
Dialysis vintage and outcomes in renal transplantation.Nephrol Dial Transplant. 2019 Apr 1;34(4):555-560. doi: 10.1093/ndt/gfy099. Nephrol Dial Transplant. 2019. PMID: 29897595 Review.
-
A single center experience of combined liver kidney transplantation.Clin Transplant. 2009 Dec;23 Suppl 21:102-14. doi: 10.1111/j.1399-0012.2009.01146.x. Clin Transplant. 2009. PMID: 19930323 Review.
Cited by
-
Kidney transplantation in Icelandic patients, 2000-2019: are outcomes affected by low volume?Front Transplant. 2024 May 28;3:1398444. doi: 10.3389/frtra.2024.1398444. eCollection 2024. Front Transplant. 2024. PMID: 38993778 Free PMC article.
-
"Long-term effects of center volume on transplant outcomes in adult kidney transplant recipients".PLoS One. 2024 Jun 6;19(6):e0301425. doi: 10.1371/journal.pone.0301425. eCollection 2024. PLoS One. 2024. PMID: 38843258 Free PMC article.
-
Association of Kidney Transplant Center Volume With 3-Year Clinical Outcomes.Am J Kidney Dis. 2019 Oct;74(4):441-451. doi: 10.1053/j.ajkd.2019.02.019. Epub 2019 May 7. Am J Kidney Dis. 2019. PMID: 31076173 Free PMC article.
-
The Effect of Transplant Volume and Patient Case Mix on Center Variation in Kidney Transplantation Outcomes.Can J Kidney Health Dis. 2019 Sep 20;6:2054358119875462. doi: 10.1177/2054358119875462. eCollection 2019. Can J Kidney Health Dis. 2019. PMID: 31565233 Free PMC article.
-
Predictive Value of HAS-BLED Score Regarding Bleeding Events and Graft Survival following Renal Transplantation.J Clin Med. 2022 Jul 12;11(14):4025. doi: 10.3390/jcm11144025. J Clin Med. 2022. PMID: 35887788 Free PMC article.
References
-
- Tonelli M, Wiebe N, Knoll G, et al. Systematic review: kidney transplantation compared with dialysis in clinically relevant outcomes. Am J Transplant. 2011;11(10):2093-2109. - PubMed
-
- Knoll G. Trends in kidney transplantation over the past decade. Drugs. 2008;(68)(suppl 1):3-10. - PubMed
-
- United States Renal Data System. Annual data report. Date unknown. http://www.usrds.org/.
-
- Legendre C, Canaud G, Martinez F. Factors influencing long-term outcome after kidney transplantation. Transpl Int. 2014;27(1):19-27. - PubMed
-
- Knoll G, Muirhead N, Trpeski L, Zhu N, Badovinac K. Patient survival following renal transplant failure in Canada. Am J Transplant. 2005;5(7):1719-1724. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
