

Associations of Dietary Protein and Energy Intakes With Protein-Energy Wasting Syndrome in Hemodialysis Patients
- PMID: 29270488
- PMCID: PMC5733766
- DOI: 10.1016/j.ekir.2017.04.002
Associations of Dietary Protein and Energy Intakes With Protein-Energy Wasting Syndrome in Hemodialysis Patients
Abstract
Introduction: The associations of dietary protein and/or energy intakes with protein or energy wasting in patients on maintenance hemodialysis are controversial. We examined these in the Hemodialysis (HEMO) Study.
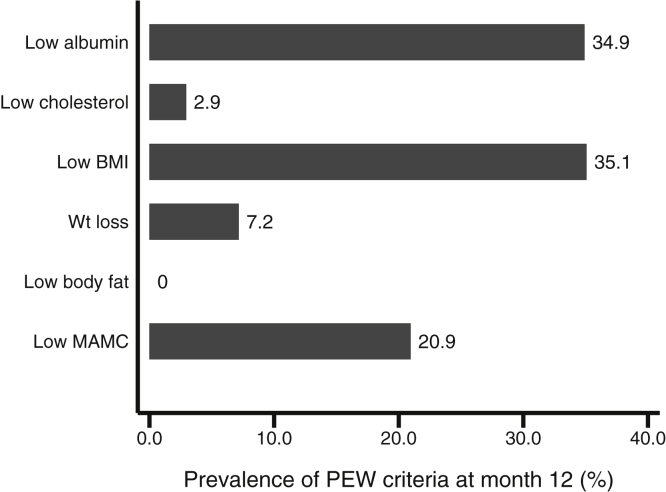
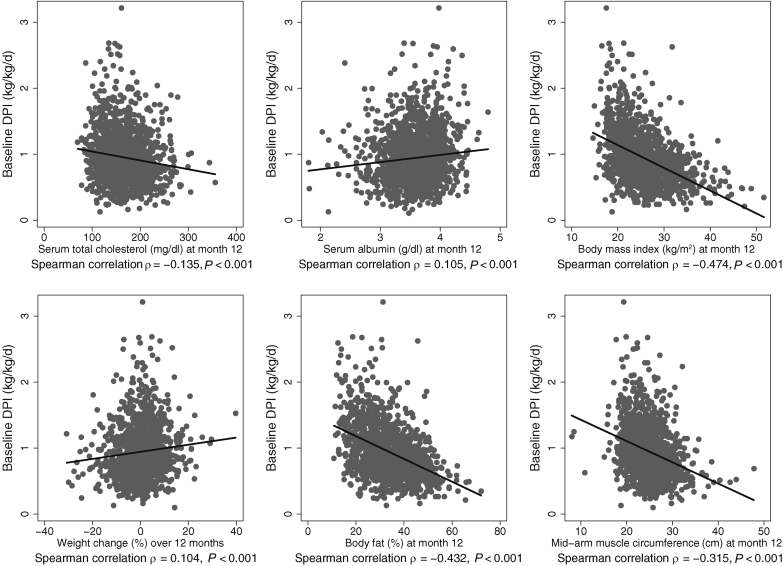
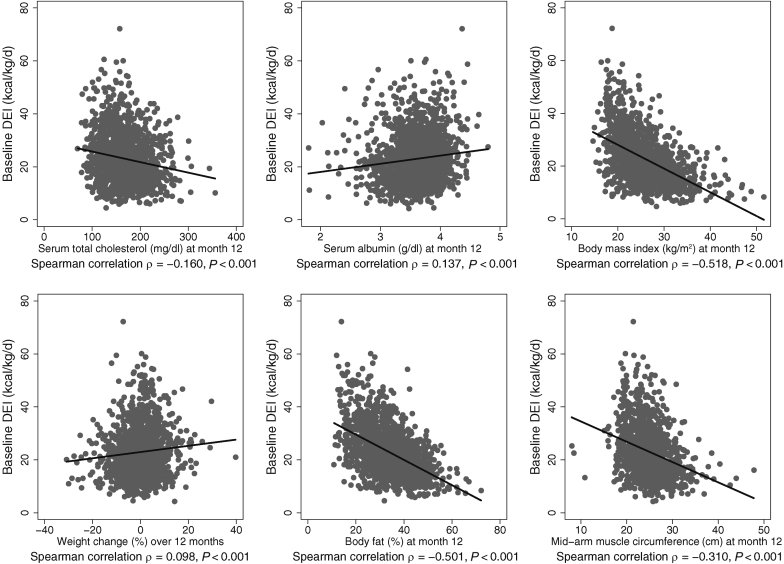
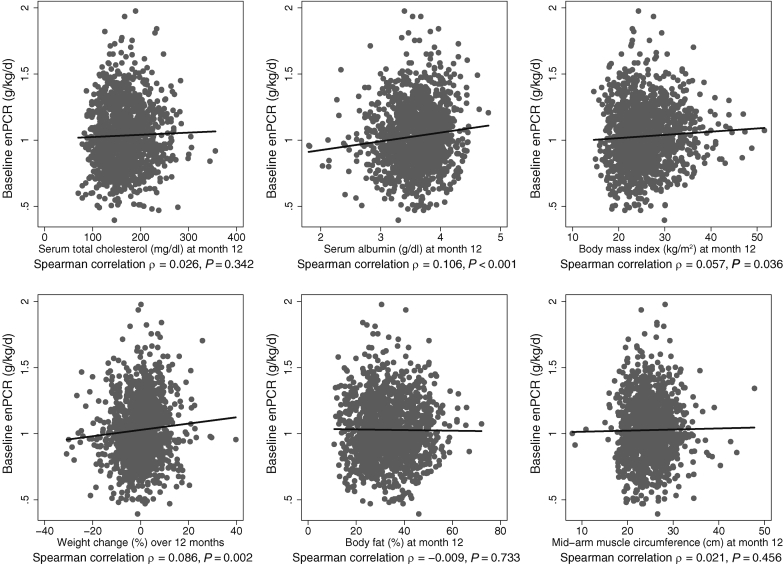
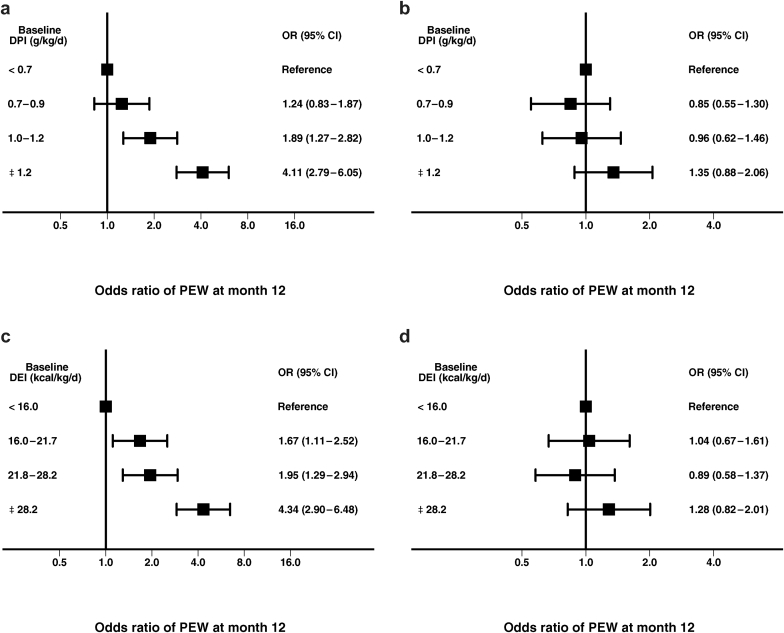
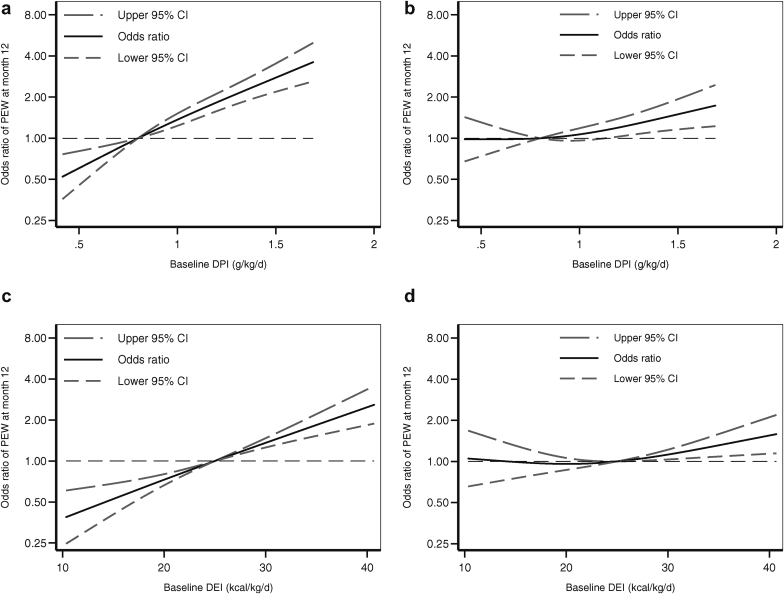
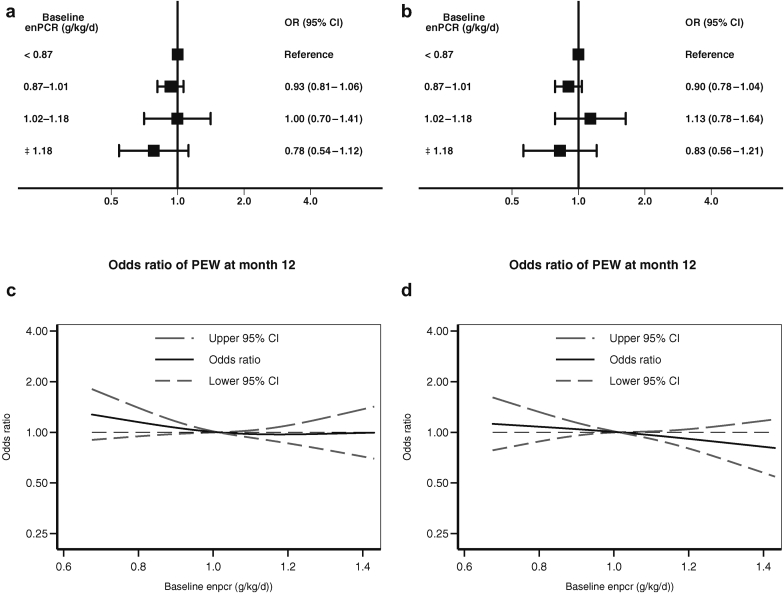
Methods: In 1487 participants in the HEMO Study, baseline dietary protein intake (grams per kilogram per day) and dietary energy intake (kilocalories per kilograms per day) were related to the presence of the protein-energy wasting (PEW) syndrome at month 12 (defined as the presence of at least 1 criteria in 2 of the 3 categories of low serum chemistry, low body mass, and low muscle mass) in logistic regression models. In additional separate models, protein intake estimated from equilibrated normalized protein catabolic rate (enPCR) was also related to the PEW syndrome.
Results: Compared with the lowest quartile, the highest quartile of baseline dietary protein intake was paradoxically associated with increased risk of the PEW syndrome at month 12 (odds ratio [OR]: 4.11; 95% confidence interval [CI]: 2.79-6.05). This relationship was completely attenuated (OR: 1.35; 95% CI: 0.88-2.06) with adjustment for baseline body weight, which suggested mathematical coupling. Results were similar for dietary energy intake. Compared with the lowest quartile of baseline enPCR, the highest quartile was not associated with the PEW syndrome at 12 months (OR: 0.78; 95% CI: 0.54-1.12).
Discussion: These data do not support the use of dietary protein intake or dietary energy intake criteria in the definition of the PEW syndrome in patients on maintenance hemodialysis.
Keywords: chronic kidney disease; hemodialysis; protein-energy wasting.
Figures
References
-
- U.S. Renal Data System: Adjusted survival probabilities, from day one, in the incident ESRD population, 2011 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2011. Available at: http://www.usrds.org/2011/view/v2_05.asp. Accessed June 14, 2017.
-
- Leavey S.F., McCullough K., Hecking E., Goodkin D., Port F.K., Young E.W. Body mass index and mortality in 'healthier' as compared with 'sicker' haemodialysis patients: results from the Dialysis Outcomes and Practice Patterns Study (DOPPS) Nephrol Dial Transplant. 2001;16:2386–2394. - PubMed
-
- Kalantar-Zadeh K., Abbott K.C., Salahudeen A.K., Kilpatrick R.D., Horwich T.B. Survival advantages of obesity in dialysis patients. Am J Clin Nutr. 2005;81:543–554. - PubMed
-
- Beddhu S., Pappas L.M., Ramkumar N., Samore M. Effects of body size and body composition on survival in hemodialysis patients. J Am Soc Nephrol. 2003;14:2366–2372. - PubMed
-
- Beddhu S., Pappas L.M., Ramkumar N., Samore M.H. Malnutrition and atherosclerosis in dialysis patients. J Am Soc Nephrol. 2004;15:733–742. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
