

Neurodevelopmental consequences of pediatric cancer and its treatment: applying an early adversity framework to understanding cognitive, behavioral, and emotional outcomes
- PMID: 29270773
- PMCID: PMC6639713
- DOI: 10.1007/s11065-017-9365-1
Neurodevelopmental consequences of pediatric cancer and its treatment: applying an early adversity framework to understanding cognitive, behavioral, and emotional outcomes
Abstract
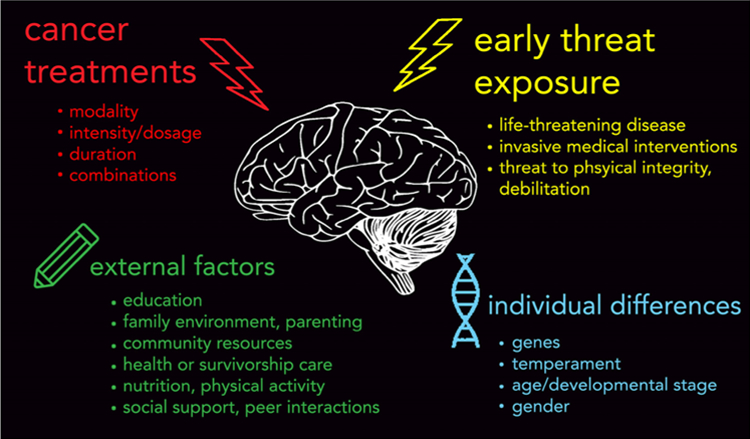
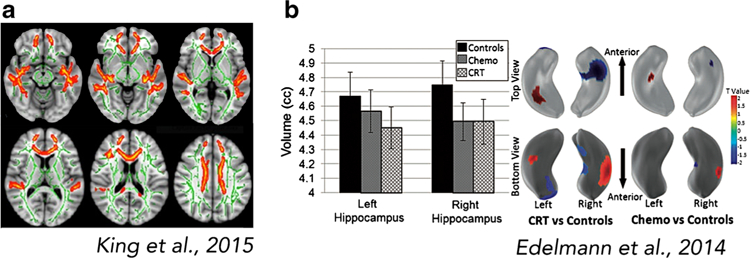
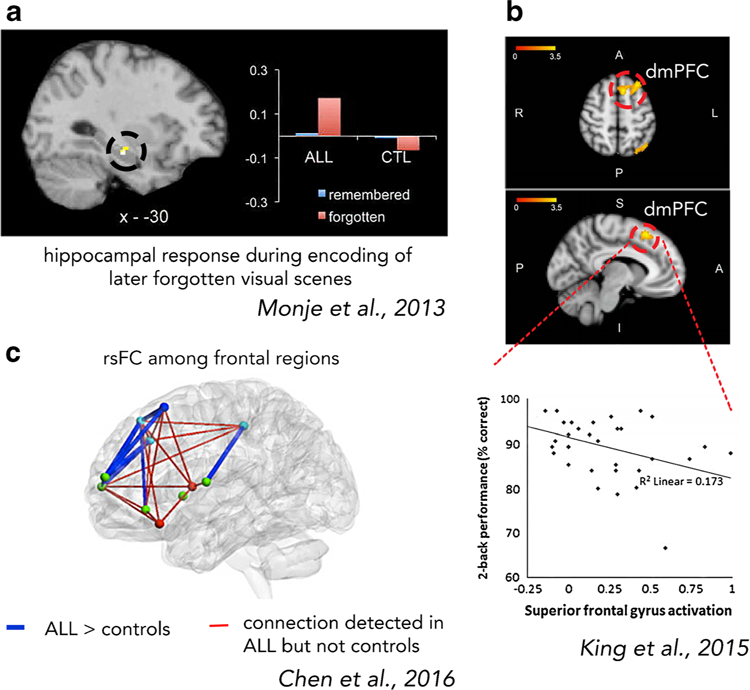
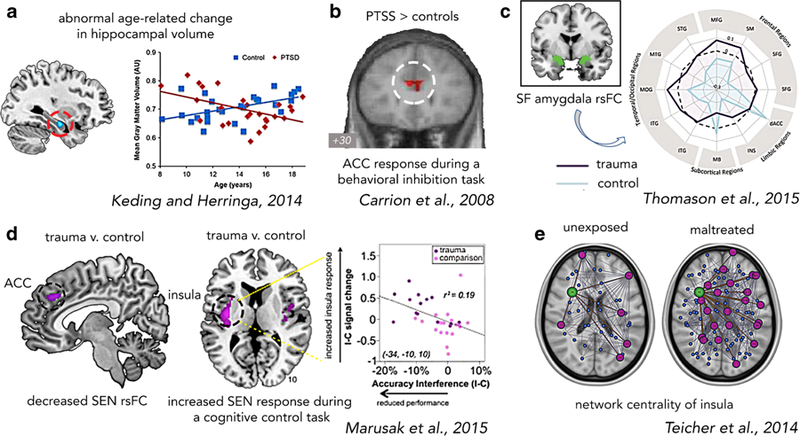
Today, children are surviving pediatric cancer at unprecedented rates, making it one of modern medicine's true success stories. However, we are increasingly becoming aware of several deleterious effects of cancer and the subsequent "cure" that extend beyond physical sequelae. Indeed, survivors of childhood cancer commonly report cognitive, emotional, and psychological difficulties, including attentional difficulties, anxiety, and posttraumatic stress symptoms (PTSS). Cognitive late- and long-term effects have been largely attributed to neurotoxic effects of cancer treatments (e.g., chemotherapy, cranial irradiation, surgery) on brain development. The role of childhood adversity in pediatric cancer - namely, the presence of a life-threatening disease and endurance of invasive medical procedures - has been largely ignored in the existing neuroscientific literature, despite compelling research by our group and others showing that exposure to more commonly studied adverse childhood experiences (i.e., domestic and community violence, physical, sexual, and emotional abuse) strongly imprints on neural development. While these adverse childhood experiences are different in many ways from the experience of childhood cancer (e.g., context, nature, source), they do share a common element of exposure to threat (i.e., threat to life or physical integrity). Therefore, we argue that the double hit of early threat and cancer treatments likely alters neural development, and ultimately, cognitive, behavioral, and emotional outcomes. In this paper, we (1) review the existing neuroimaging research on child, adolescent, and adult survivors of childhood cancer, (2) summarize gaps in our current understanding, (3) propose a novel neurobiological framework that characterizes childhood cancer as a type of childhood adversity, particularly a form of early threat, focusing on development of the hippocampus and the salience and emotion network (SEN), and (4) outline future directions for research.
Keywords: Childhood cancer; brain; brain tumor; leukemia; pediatric oncology.
Figures

References
-
- Aber JL, Bennett NG, Conley DC, & Li J (1997). The effects of poverty on child health and development. Annual review of public health, 18(1), 463–483. - PubMed
-
- Ainsworth MS (1979). Infant–mother attachment. American psychologist, 34(10), 932. - PubMed
-
- Alderfer MA, & Kazak AE (2006). Family issues when a child is on treatment for cancer. In Comprehensive handbook of childhood cancer and sickle cell disease: A biopsychosocial approach (pp. 53–74). New York: Oxford University Press.
-
- Alderfer MA, Labay LE, & Kazak AE (2003). Brief report: does posttraumatic stress apply to siblings of childhood cancer survivors? Journal of pediatric psychology, 28(4), 281–286. - PubMed
Publication types
MeSH terms
Grants and funding
- 14-238-04-IRG/American Cancer Society (US)/International
- 129368-PF-16-057-01-PCSM/American Cancer Society (US)/International
- K01 MH101123/MH/NIMH NIH HHS/United States
- K01MH101123/National Institute of Mental Health (US)/International
- R61MH111935/National Institute of Mental Health (US)/International
LinkOut - more resources
Full Text Sources
Other Literature Sources
