

Community-Acquired Pneumonia in Adults
- PMID: 29271341
- PMCID: PMC5754574
- DOI: 10.3238/arztebl.2017.0838
Community-Acquired Pneumonia in Adults
Abstract
Background: The clinical spectrum of community-acquired pneumonia ranges from infections that can be treated on an outpatient basis, with 1% mortality, to those that present as medical emergencies, with a mortality above 40%.
Methods: This article is based on pertinent publications and current guidelines retrieved by a selective search of the literature.
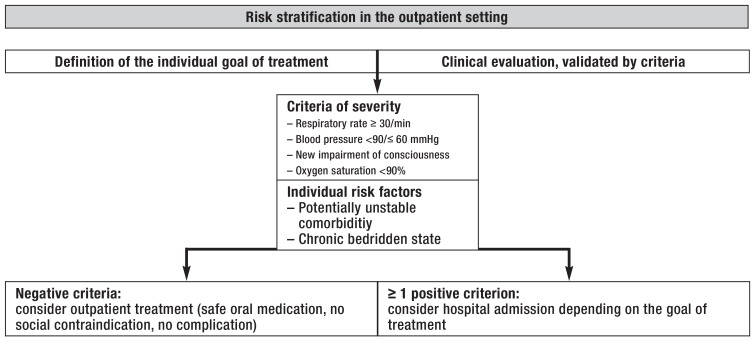
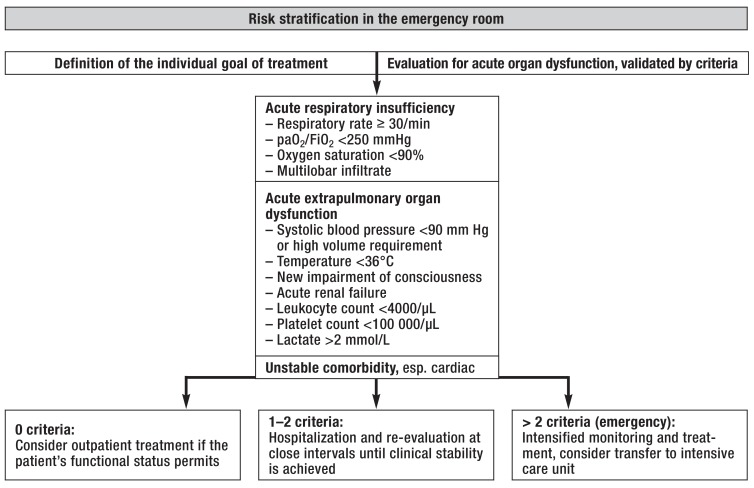
Results: The radiological demonstration of an infiltrate is required for the differentiation of pneumonia from acute bronchitis regardless of whether the patient is seen in the outpatient setting or in the emergency room. For risk prediction, it is recommended that the CRB-65 criteria, unstable comorbidities, and oxygenation should be taken into account. Amoxicillin is the drug of choice for mild pneumonia; it should be given in combination with clavulanic acid if there are any comorbid illnesses. The main clinical concerns in the emergency room are the identification of acute organ dysfunction and the management of sepsis. Intravenous beta-lactam antibiotics should be given initially, in combination with a macrolide if acute organ dysfunction is present. The treatment should be continued for 5-7 days. Cardiovascular complications worsen the patient's prognosis and should be meticulously watched for. Structured followup care includes the follow-up of comorbid conditions and the initiation of recommended preventive measures such as antipneumococcal and anti-influenza vaccination, the avoidance of drugs that increase the risk, smoking cessation, and treatment of dysphagia, if present.
Conclusion: Major considerations include appropriate risk stratification and the implementation of a management strategy adapted to the degree of severity of the disease, along with the establishment of structured follow-up care and secondary prevention, especially for patients with comorbidities.
Figures

Comment in
-
Adequate Risk Stratification.Dtsch Arztebl Int. 2018 Mar 2;115(9):145. doi: 10.3238/arztebl.2018.0145a. Dtsch Arztebl Int. 2018. PMID: 29563010 Free PMC article. No abstract available.
References
-
- Murray CJ, Lopez AD. Measuring the global burden of disease. N Engl J Med. 2013;369:448–457. - PubMed
-
- Kolditz M, Tesch F, Mocke L, Hoffken G, Ewig S, Schmitt J. Burden and risk factors of ambulatory or hospitalized CAP: a population based cohort study. Respir Med. 2016;121:32–38. - PubMed
-
- Kolditz M, Bauer TT, Konig T, Rohde G, Ewig S. 3-day mortality in hospitalised community-acquired pneumonia: frequency and risk factors. Eur Respir J. 2016;47:1572–1574. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical