

Pelvic floor muscle training for prevention and treatment of urinary and faecal incontinence in antenatal and postnatal women
- PMID: 29271473
- PMCID: PMC6486304
- DOI: 10.1002/14651858.CD007471.pub3
Pelvic floor muscle training for prevention and treatment of urinary and faecal incontinence in antenatal and postnatal women
Update in
-
Pelvic floor muscle training for preventing and treating urinary and faecal incontinence in antenatal and postnatal women.Cochrane Database Syst Rev. 2020 May 6;5(5):CD007471. doi: 10.1002/14651858.CD007471.pub4. Cochrane Database Syst Rev. 2020. PMID: 32378735 Free PMC article.
Abstract
Background: About one-third of women have urinary incontinence and up to one-tenth have faecal incontinence after childbirth. Pelvic floor muscle training (PFMT) is commonly recommended during pregnancy and after birth for both prevention and treatment of incontinence.This is an update of a review previously published in 2012.
Objectives: To determine the effectiveness of pelvic floor muscle training (PFMT) in the prevention or treatment of urinary and faecal incontinence in pregnant or postnatal women.
Search methods: We searched the Cochrane Incontinence Specialised Register (16 February 2017) and reference lists of retrieved studies.
Selection criteria: Randomised or quasi-randomised trials in pregnant or postnatal women. One arm of the trial included PFMT. Another arm was no PFMT, usual antenatal or postnatal care, another control condition, or an alternative PFMT intervention.
Data collection and analysis: Review authors independently assessed trials for inclusion and risk of bias. We extracted data and checked them for accuracy. Populations included: women who were continent (PFMT for prevention), women who were incontinent (PFMT for treatment) at randomisation and a mixed population of women who were one or the other (PFMT for prevention or treatment). We assessed quality of evidence using the GRADE approach.
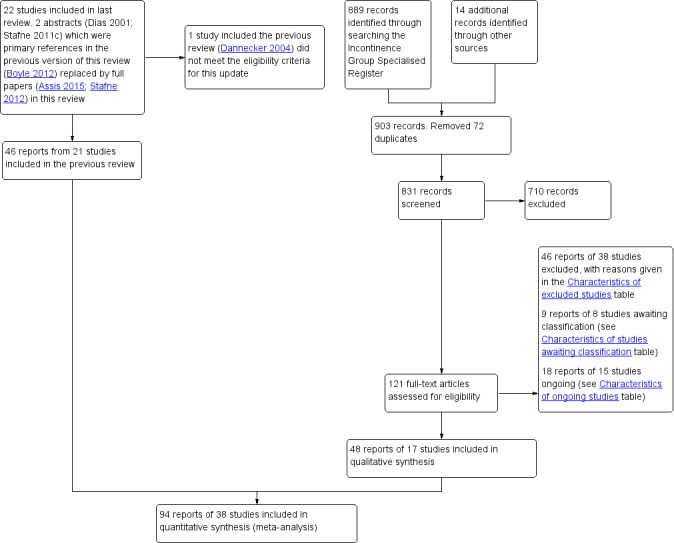
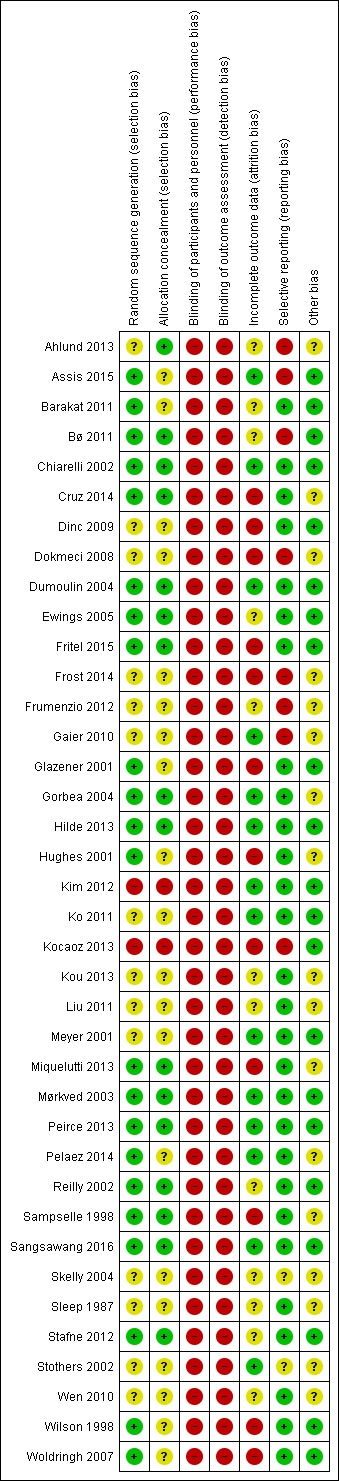
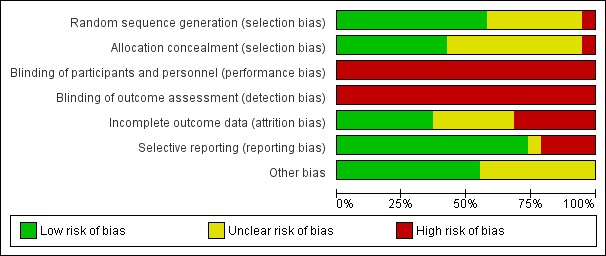
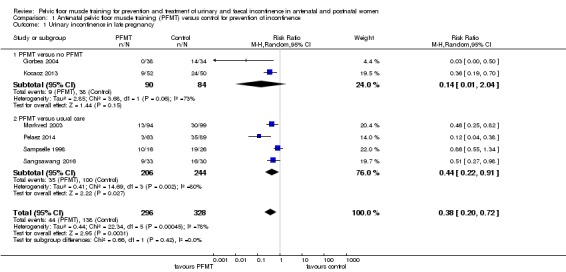
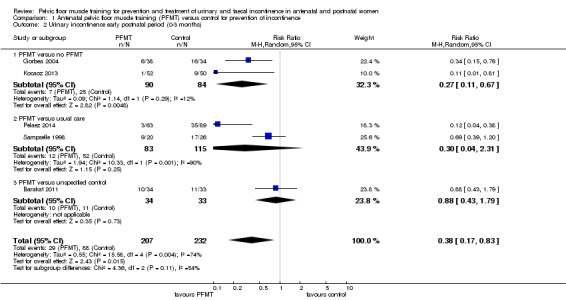
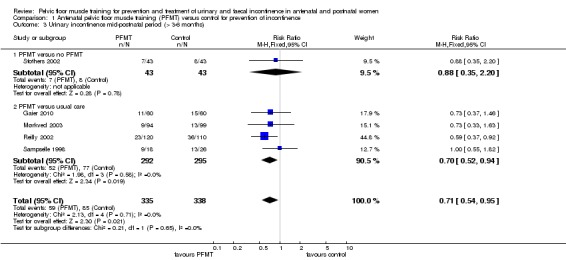
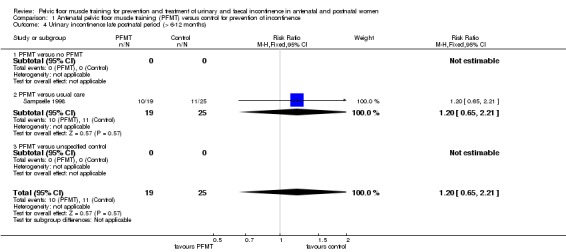
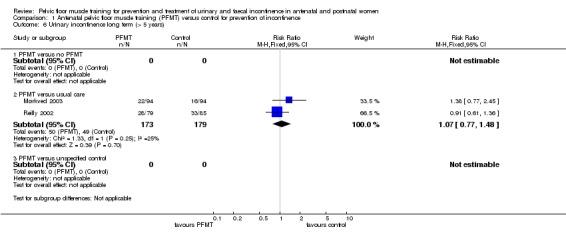
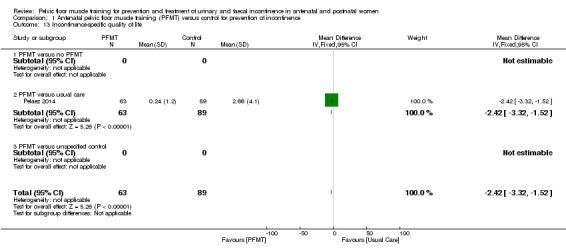
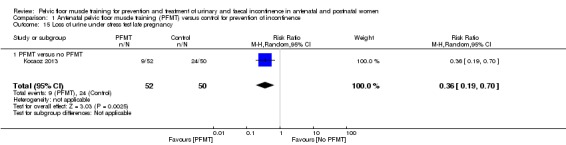
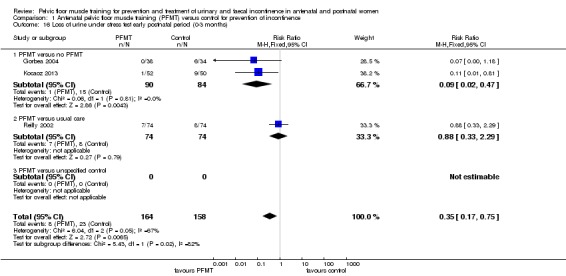
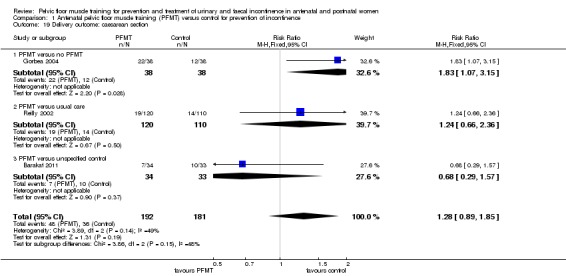
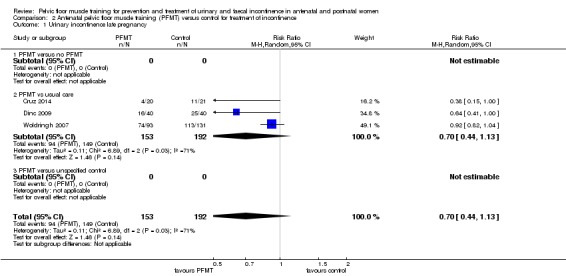
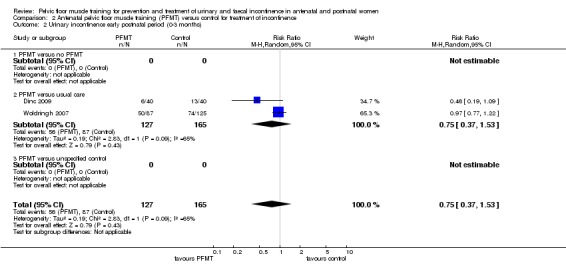
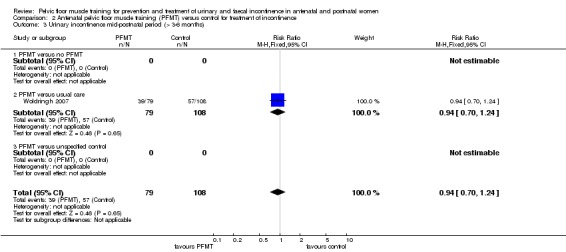
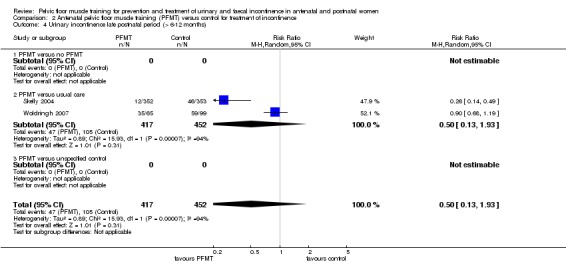
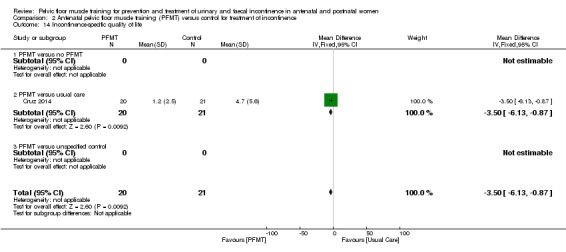
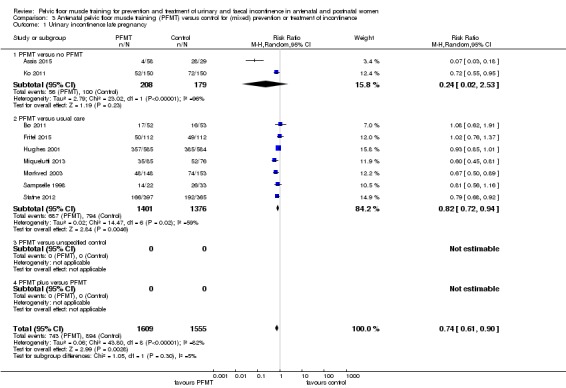
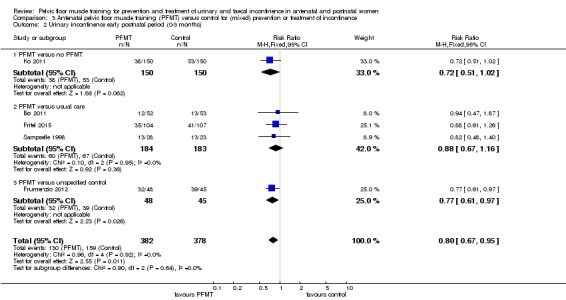
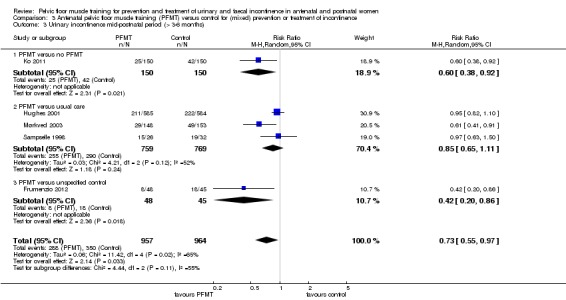
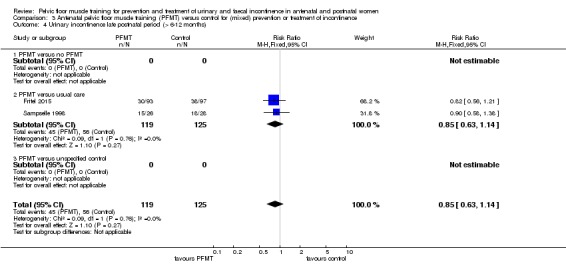
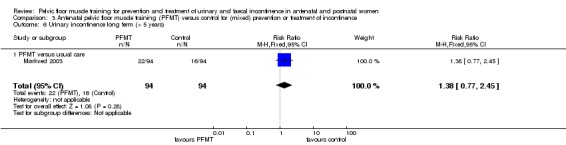
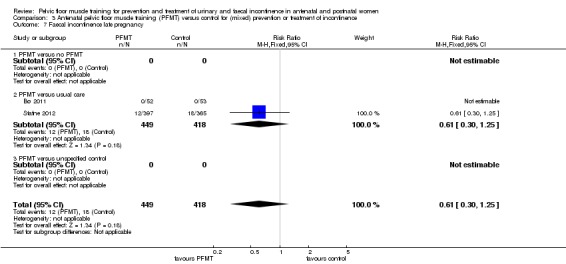
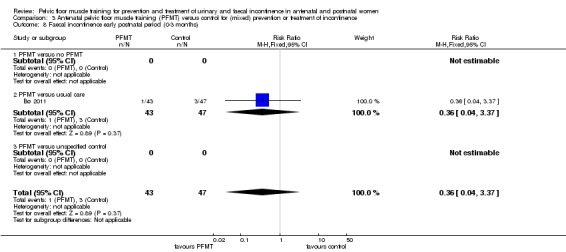
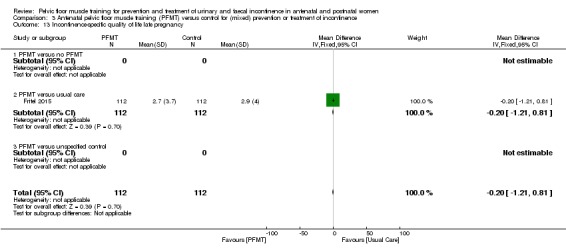
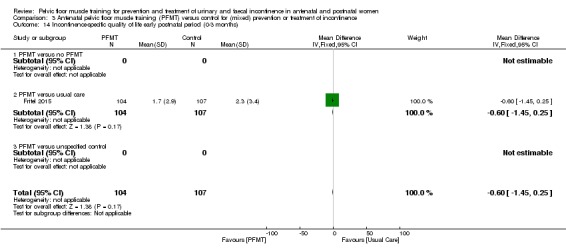
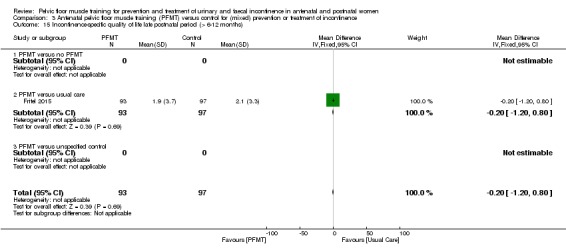
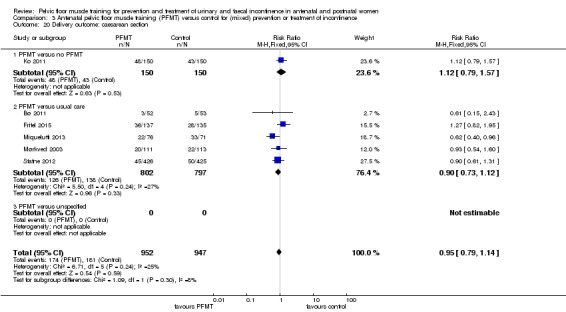
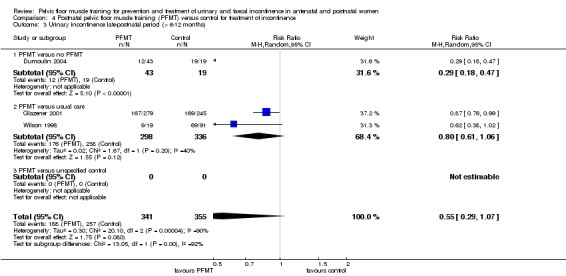
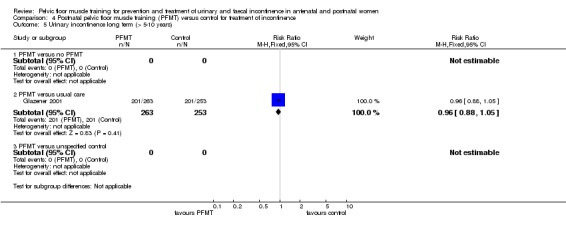
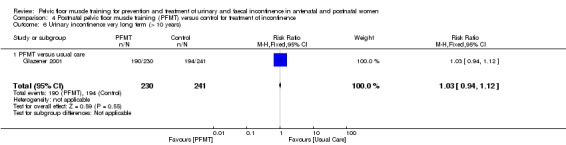
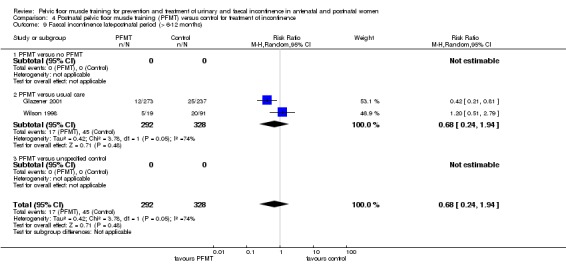
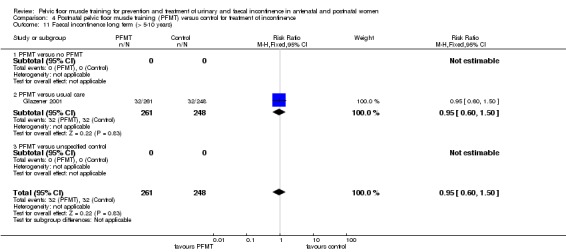
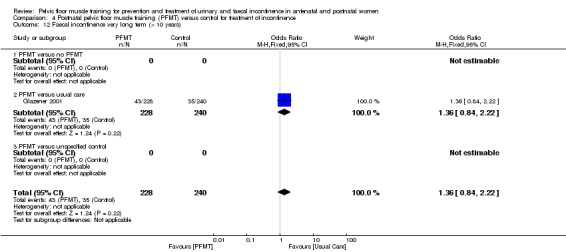
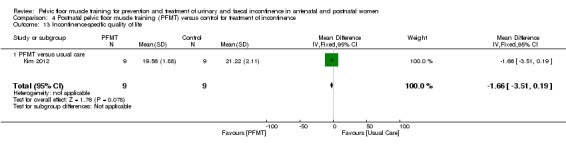
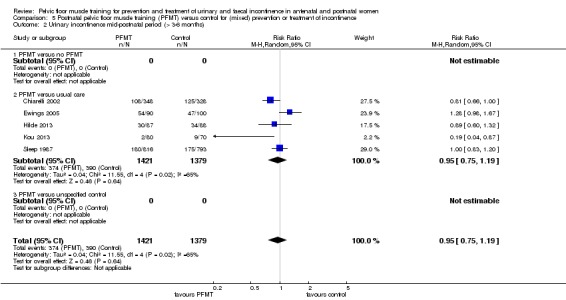
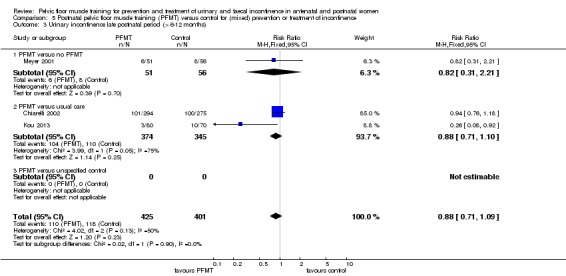
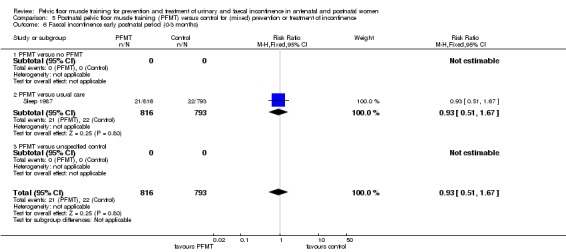
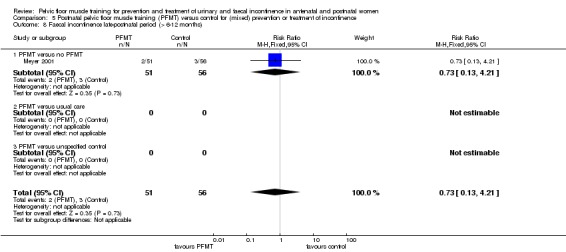
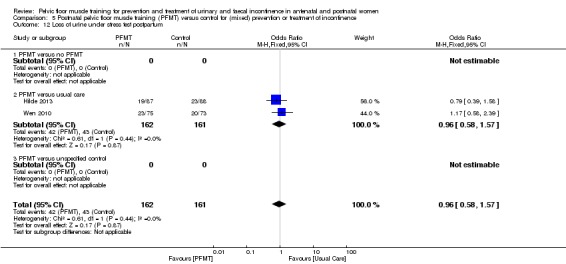
Main results: The review included 38 trials (17 of which were new for this update) involving 9892 women from 20 countries. Overall, trials were small to moderate sized, and the PFMT programmes and control conditions varied considerably and were often poorly described. Many trials were at moderate to high risk of bias. Other than two reports of pelvic floor pain, trials reported no harmful effects of PFMT.Prevention of urinary incontinence: compared with usual care, continent pregnant women performing antenatal PFMT may have had a lower risk of reporting urinary incontinence in late pregnancy (62% less; risk ratio (RR) for incontinence 0.38, 95% confidence interval (CI) 0.20 to 0.72; 6 trials, 624 women; low-quality evidence). Similarly, antenatal PFMT decreased the risk of urinary incontinence in the mid-postnatal period (more than three to six months' postpartum) (29% less; RR 0.71, 95% CI 0.54 to 0.95; 5 trials, 673 women; moderate-quality evidence). There was insufficient information available for the late (more than six to 12 months') postnatal period to determine effects at this time point.Treatment of urinary incontinence: it is uncertain whether antenatal PFMT in incontinent women decreases incontinence in late pregnancy compared to usual care (RR 0.70, 95% CI 0.44 to 1.13; 3 trials, 345 women; very low-quality evidence). This uncertainty extends into the mid- (RR 0.94, 95% CI 0.70 to 1.24; 1 trial, 187 women; very low-quality evidence) and late (RR 0.50, 95% CI 0.13 to 1.93; 2 trials, 869 women; very low-quality evidence) postnatal periods. In postnatal women with persistent urinary incontinence, it was unclear whether PFMT reduced urinary incontinence at more than six to 12 months' postpartum (RR 0.55, 95% CI 0.29 to 1.07; 3 trials; 696 women; very low-quality evidence).Mixed prevention and treatment approach to urinary incontinence: antenatal PFMT in women with or without urinary incontinence (mixed population) may decrease urinary incontinence risk in late pregnancy (26% less; RR 0.74, 95% CI 0.61 to 0.90; 9 trials, 3164 women; low-quality evidence) and the mid-postnatal period (RR 0.73, 95% CI 0.55 to 0.97; 5 trials, 1921 women; very low-quality evidence). It is uncertain if antenatal PFMT reduces urinary incontinence risk late postpartum (RR 0.85, 95% CI 0.63 to 1.14; 2 trials, 244 women; low-quality evidence). For PFMT begun after delivery, there was considerable uncertainty about the effect on urinary incontinence risk in the late postnatal period (RR 0.88, 95% CI 0.71 to 1.09; 3 trials, 826 women; very low-quality evidence).Faecal incontinence: six trials reported faecal incontinence outcomes. In postnatal women with persistent faecal incontinence, it was uncertain whether PFMT reduced incontinence in the late postnatal period compared to usual care (RR 0.68, 95% CI 0.24 to 1.94; 2 trials; 620 women; very low-quality evidence). In women with or without faecal incontinence (mixed population), antenatal PFMT led to little or no difference in the prevalence of faecal incontinence in late pregnancy (RR 0.61, 95% CI 0.30 to 1.25; 2 trials, 867 women; moderate-quality evidence). For postnatal PFMT in a mixed population, there was considerable uncertainty about the effect on faecal incontinence in the late postnatal period (RR 0.73, 95% CI 0.13 to 4.21; 1 trial, 107 women, very low-quality evidence).There was little evidence about effects on urinary or faecal incontinence beyond 12 months' postpartum. There were few incontinence-specific quality of life data and little consensus on how to measure it. We found no data on health economics outcomes.
Authors' conclusions: Targeting continent antenatal women early in pregnancy and offering a structured PFMT programme may prevent the onset of urinary incontinence in late pregnancy and postpartum. However, the cost-effectiveness of this is unknown. Population approaches (recruiting antenatal women regardless of continence status) may have a smaller effect on urinary incontinence, although the reasons for this are unclear. It is uncertain whether a population-based approach for delivering postnatal PFMT is effective in reducing urinary incontinence. Uncertainty surrounds the effects of PFMT as a treatment for urinary incontinence in antenatal and postnatal women, which contrasts with the more established effectiveness in mid-life women.It is possible that the effects of PFMT might be greater with targeted rather than mixed prevention and treatment approaches and in certain groups of women. Hypothetically, for instance, women with a high body mass index are at risk factor for urinary incontinence. Such uncertainties require further testing and data on duration of effect are also needed. The physiological and behavioural aspects of exercise programmes must be described for both PFMT and control groups and how much PFMT women in both groups do, to increase understanding of what works and for whom.Few data exist on faecal incontinence or costs and it is important that both are included in any future trials. It is essential that future trials use valid measures of incontinence-specific quality of life for both urinary and faecal incontinence.
Conflict of interest statement
SW: none known. RB: none known. JC: none known. SM: was an investigator on two of the included trials in the review and had no role in screening, quality assessment or data extraction for these trials. JHS: none known.
Figures
Update of
-
Pelvic floor muscle training for prevention and treatment of urinary and faecal incontinence in antenatal and postnatal women.Cochrane Database Syst Rev. 2012 Oct 17;10:CD007471. doi: 10.1002/14651858.CD007471.pub2. Cochrane Database Syst Rev. 2012. Update in: Cochrane Database Syst Rev. 2017 Dec 22;12:CD007471. doi: 10.1002/14651858.CD007471.pub3. PMID: 23076935 Updated.
References
References to studies included in this review
-
- Ahlund S, Nordgren B, Wilander EL, Wiklund I, Friden C. Is home‐based pelvic floor muscle training effective in treatment of urinary incontinence after birth in primiparous women? A randomized controlled trial. Acta Obstetricia et Gynecologica Scandinavica 2013;92(8):909‐15. [sr‐incont48416] - PubMed
-
- Assis LC, Bernardes JM, Barbosa AM, Santini AC, Vianna LS, Dias A. Effectiveness of an illustrated home exercise guide on promoting urinary continence during pregnancy: a pragmatic randomized clinical trial [Portuguese]. Revista Brasileira de Ginecologia e Obstetricia 2015;37(10):460‐6. [sr‐incont69254] - PubMed
- Assis LC, Dias A, Barbosa AMP, Santini ACM, Sousa VO, Vianna LS, et al. Contribution of early intensive prolonged pelvic floor exercises (Abstract number 782‐S). American Journal of Epidemiology 2011;173(Suppl 11):S196. [sr‐incont47327]
- Dias A, Assis L, Barbosa A, Santini AC, Picelli‐Dias F. Effectiveness of perineal exercises in controlling urinary incontinence and improving pelvic floor muscle function during pregnancy (Abstract number 117). Neurourology and Urodynamics 2011;30(6):968.
-
- Barakat R, Pelaez M, Montejo R, Luaces M, Zakynthinaki M. Exercise during pregnancy improves maternal health perception: a randomized controlled trial. American Journal of Obstetrics and Gynecology 2011;204(5):402.e1‐7. [sr‐incont65194] - PubMed
-
- Bø K, Haakstad L. Is pelvic floor muscle training effective when taught in a general fitness class for pregnant women? A randomized controlled trial (Abstract number 200). International Urogynecology Journal 2009;20(Suppl 2):S238‐9.
- Bø K, Haakstad LA. Is pelvic floor muscle training effective when taught in a general fitness class in pregnancy? A randomised controlled trial. Physiotherapy 2011;97(3):190‐5. - PubMed
-
- Chiarelli P, Cockburn J. Preventing urinary incontinence in postpartum women (Abstract). Neurourology and Urodynamics 2001;20(4):448‐9. [SR‐INCONT12109]
- Chiarelli P, Cockburn J. Promoting urinary continence in women after delivery: randomised controlled trial (extended electronic version). BMJ 2002;324:1‐6. [SR‐INCONT14669] - PMC - PubMed
- Chiarelli P, Murphy B, Cockburn J. Acceptability of a urinary continence promotion programme to women in postpartum. BJOG 2003;110(2):188‐96. [SR‐INCONT15783] - PubMed
- Chiarelli P, Murphy B, Cockburn J. Promoting urinary continence in postpartum women: 12‐month follow‐up data from a randomised controlled trial. International Urogynecology Journal 2004;15(2):99‐105. [SR‐INCONT17410] - PubMed
References to studies excluded from this review
-
- Agur W, Freeman R. Do antenatal pelvic floor training affect the outcome of labour? A randomised controlled trial (Abstract). Neurourology and Urodynamics 2005;24(5/6):510‐1. [SR‐INCONT20969] - PubMed
-
- Assis TR, Sa AC, Amaral WN, Batista EM, Formiga CK, Conde DM. The effect of an exercise program to strengthen pelvic floor muscles in multiparous women [Portuguese]. Revista Brasileira de Ginecologia e Obstetricia 2013;35(1):10‐5. - PubMed
-
- Barakat R, Perales M, Bacchi M, Coteron J, Refoyo I. A program of exercise throughout pregnancy. Is it safe to mother and newborn?. American Journal of Health Promotion 2014;29(1):2‐8. - PubMed
-
- Barakat R, Pelaez M, Cordero Y, Perales M, Lopez C, Coteron J, et al. Exercise during pregnancy protects against hypertension and macrosomia: randomized clinical trial. American Journal of Obstetrics and Gynecology 2016;214(5):649‐8. - PubMed
-
- Culligan P, Blackwell L, Murphy M, Ziegler C, Heit M. A blinded, sham‐controlled trial of postpartum extracorporeal magnetic innervation to restore pelvic muscle strength in primiparous patients (Abstract). Neurourology and Urodynamics 2004;23(5/6):451. [SR‐INCONT19008] - PubMed
- Culligan PJ, Blackwell L, Murphy M, Ziegler C, Heit MH. A randomized, double‐blinded, sham‐controlled trial of postpartum extracorporeal magnetic innervation to restore pelvic muscle strength in primiparous patients. American Journal of Obstetrics and Gynecology 2005;192(5):1578‐82. - PubMed
References to studies awaiting assessment
-
- Han V, Hyakutake M, Cundiff G, Koenig N, Baerg L, Lee T, et al. Pregnancy‐associated pelvic floor health knowledge and reduction of symptoms: the PREPARED trial (Abstract number O‐GYN‐JM‐017). Journal of Obstetrics and Gynaecology Canada 2016;38(5):487. - PubMed
- Koenig N. PREgnancy‐associated Pelvic Floor Health Knowledge And REDuction of Symptoms: the PREPARED trial. clinicaltrials.gov/show/NCT02947282 Date first received: 27 October 2016. - PubMed
-
- Johannessen HH, Wibe A, Stordahl A, Sandvik L, Mørkved S. Do pelvic floor muscle exercises reduce postpartum anal incontinence? A randomised controlled trial. BJOG 2017;124(4):686‐94. - PubMed
-
- Longo F, Montironi PL, Bar E, Frigerio S. Effects of pelvic floor muscle training during pregnancy. Techniques in Coloproctology 2013;17(1):143‐4.
-
- Oakley SH, Ghodsi VC, Crisp CC, Estanol MV, Westermann LB, Novicki KM, et al. Effects of physical therapy on pelvic floor symptoms and quality of life in postpartum women following severe perineal trauma: a randomized controlled trial. Female Pelvic Medicine & Reconstructive Surgery 2015;21(5 Suppl 1):S18.
- Oakley SH, Ghodsi VC, Crisp CC, Estanol MV, Westermann LB, Novicki KM, et al. Impact of pelvic floor physical therapy on quality of life and function after obstetric anal sphincter injury: a randomized controlled trial. Female Pelvic Medicine and Reconstructive Surgery 2016;22:205‐13. - PubMed
-
- Sun Z, Zhu L, Lang J, Zhang Y, Liu G, Chen X, et al. Postpartum pelvic floor rehabilitation on prevention of female pelvic floor dysfunction: a multicenter prospective randomized controlled study. [Chinese]. Chung‐Hua Fu Chan Ko Tsa Chih [Chinese Journal of Obstetrics and Gynecology] 2015;50(6):420‐7. - PubMed
References to ongoing studies
-
- Ferreira CHJ, Cavalcanti DLC. Effects of pelvic floor muscle training on pelvic floor muscle function in women during their first pregnancies measured by perineometer. anzctr.org.au/ACTRN12609001005246.aspx Date first received: 10 October 2009.
-
- Berghmans B. Long term effects of multidisciplinary assessment and pre‐ and post partum Pelvic Floor Muscle Group Treatment in primigravid with stress urinary incontinence compared to care‐as‐usual: a randomised controlled trial ‐ motherfit. trialregister.nl/trialreg/admin/rctview.asp?TC=5971 Date first received: 18 July 2016.
-
- Buen M. Clinical trial: influence of the practice of Pilates on the incidence of urinary incontinence, perineal strength low back pain in the third trimester. ensaiosclinicos.gov.br/rg/RBR‐4wkr8y/ Date first received: 9 April 2014.
-
- Haruna M, Asai Y. Effect of postpartum pelvic floor muscle training with ultrasound biofeedback on recovery of pelvic floor muscle function: a randomized controlled trial. UMIN Clinical Trials Registry (UMIN‐CTR) (available at: umin.ac.jp/ctr/index.htm) Date first received: 8 December 2014.
-
- Miheso J, Ngugi S. Effect of pelvic floor muscle training among pregnant black African population on the risk of postpartum urinary incontinence, a single blind randomized control trial. Pan African Clinical Trials Registry (PACTR) (available at: pactr.org) Date first received: 22 May 2014.
- Ngugi S. Effect of Pelvic Floor Muscle Training Among Pregnant Black African Population on the Risk of Postpartum Urinary Incontinence, a Single Blind Randomized Control Trial [Masters dissertation]. Nairobi (Kenya): Aga Khan University (Nairobi Campus), 2015.
Additional references
-
- Abrams P, Andersson K‐E, Apostolidis A, Birder L, Bliss D, Brubaker L, et al. Evaluation and treatment of urinary incontinence, pelvic organ prolapse and faecal incontinence: recommendations of the International Scientific Committee, 6th International Consultation on Incontinence. In: Abrams P, Cardozo L, Wagg A, Wein A editor(s). Incontinence: 6th International Consultation on Incontinence, Tokyo, September 2016. 6th Edition. Vol. 1, Bristol (UK): International Continence Society (ICS) and International Consultation on Urological Diseases (ICUD), 2017:2549‐619.
-
- Avery K, Donovan J, Peters TJ, Shaw C, Gotoh M, Abrams P. ICIQ: a brief and robust measure for evaluating the symptoms and impact of urinary incontinence. Neurourology and Urodynamics 2004;23:322‐30. - PubMed
-
- Avery KN, Bosch JL, Gotoh M, Naughton M, Jackson S, Radley SC, et al. Questionnaires to assess urinary and anal incontinence: review and recommendations. Journal of Urology 2007;177:39‐49. - PubMed
-
- Bols EM, Hendriks EJ, Berghmans BC, Baeten CG, Nijhuis JG, Bie RA. A systematic review of etiological factors for postpartum fecal incontinence. Acta Obstetricia et Gynecologica Scandinavica 2010;89(3):302‐14. - PubMed
References to other published versions of this review
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical