

Higher-than-expected prevalence of non-tuberculous mycobacteria in HIV setting in Botswana: Implications for diagnostic algorithms using Xpert MTB/RIF assay
- PMID: 29272273
- PMCID: PMC5741233
- DOI: 10.1371/journal.pone.0189981
Higher-than-expected prevalence of non-tuberculous mycobacteria in HIV setting in Botswana: Implications for diagnostic algorithms using Xpert MTB/RIF assay
Abstract
Background: Non-tuberculous mycobacteria (NTM) can cause pulmonary infection and disease especially among people living with HIV (PLHIV). PLHIV with NTM disease may clinically present with one of the four symptoms consistent with tuberculosis (TB). We describe the prevalence of NTM and Mycobacterium tuberculosis complex (MTBC) isolated among PLHIV who presented for HIV care and treatment.
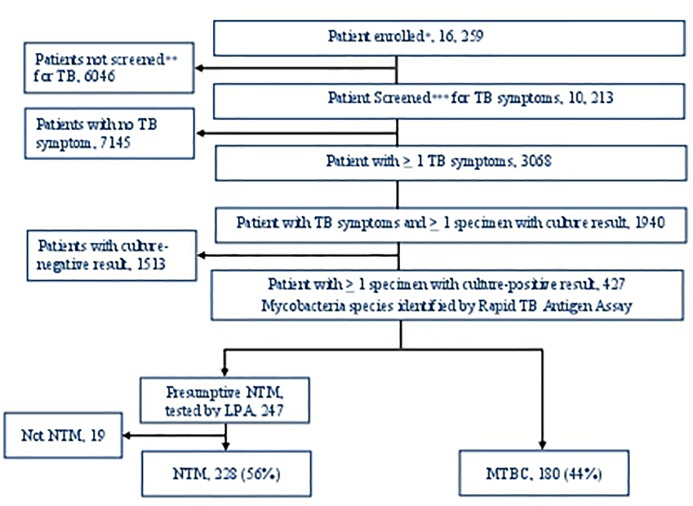
Methods: All PLHIV patients presenting for HIV care and treatment services at 22 clinical sites in Botswana were offered screening for TB and were recruited. Patients who had ≥1 TB symptom were asked to submit sputa for Xpert MTB/RIF and culture. Culture growth was identified as NTM and MTBC using the SD-Bioline TB Ag MPT64 Kit and Ziehl Neelsen microscopy. NTM and MTBC isolates underwent species identification by the Hain GenoType CM and AS line probe assays.
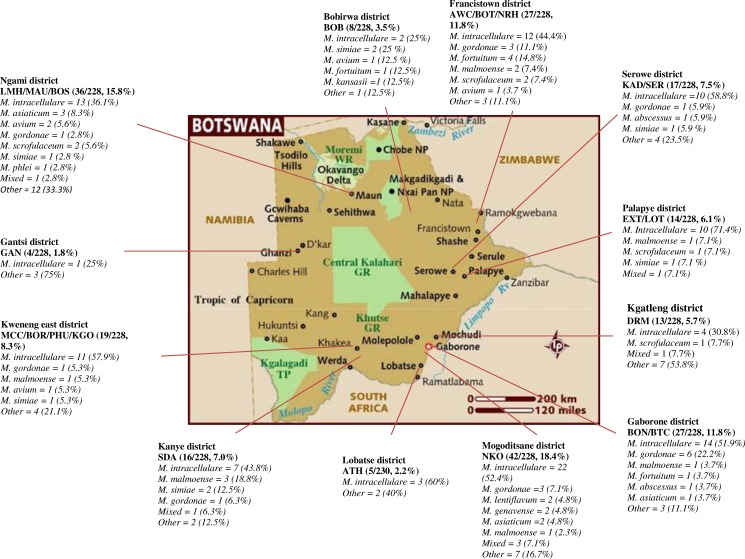
Results: Among 16, 259 PLHIV enrolled 3068 screened positive for at least one TB symptom. Of these, 1940 submitted ≥1 sputum specimen, 427 (22%) patients had ≥1 positive-culture result identified phenotypically for mycobacterial growth. Of these 247 and 180 patients were identified as having isolates were NTM and MTBC, respectively. Of the 247 patients identified with isolates containing NTM; 19 were later excluded as not having NTM based on additional genotypic testing. Among the remaining 408 patients 228 (56%, 95% confidence interval, 46-66%) with NTM. M. intracellulare was the most common isolated (47.8%). Other NTMs commonly associated with pulmonary disease included M. malmoense (3.9%), M. avium (2.2%), M. abscessus (0.9%) and M. kansasii (0.4%). After excluding NTM isolates that were non-speciated and M. gordonae 154 (67.5%) of the NTM isolates were potential pathogens.
Conclusions: In the setting of HIV care and treatment, over-half (56%) of a positive sputum culture among PLHIV with TB symptoms was NTM. Though we were not able to distinguish in our study NTM disease and colonization, the study suggests culture and species identification for PLHIV presenting with TB symptoms remains important to facilitate NTM diagnosis and hasten time to appropriate treatment.
Conflict of interest statement
Figures
References
-
- Brode S.K, Daley C.L and Marras T.K. The epidemiologic relationship between tuberculosis and nontuberculous mycobacterial disease: a systematic review. Int J Tuberc Lung Dis. 2014. - PubMed
-
- Sonnenberg P, Murray J, Glynn J.R, Thomas R, Godfrey-Faussett, Shearer S. Risk factors for pulmonary disease due to culture-positive MTB or NTM in South African gold miners Eur Respir J 2000-15-291–296.. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
