

Wildland fire smoke and human health
- PMID: 29272827
- PMCID: PMC6697173
- DOI: 10.1016/j.scitotenv.2017.12.086
Wildland fire smoke and human health
Abstract
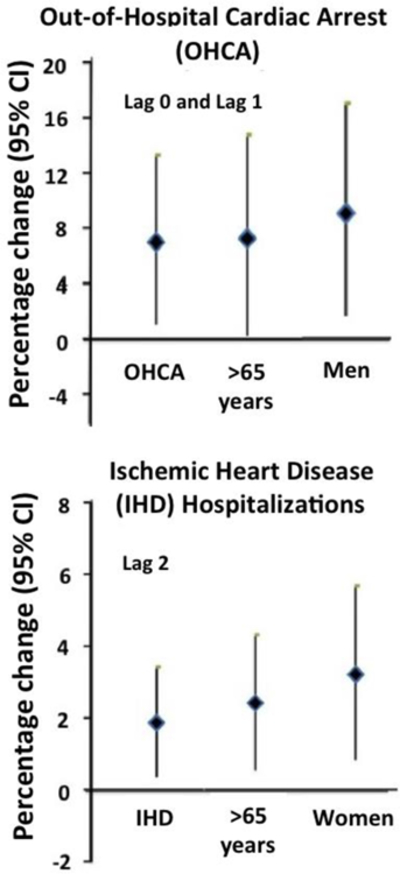
The natural cycle of landscape fire maintains the ecological health of the land, yet adverse health effects associated with exposure to emissions from wildfire produce public health and clinical challenges. Systematic reviews conclude that a positive association exists between exposure to wildfire smoke or wildfire particulate matter (PM2.5) and all-cause mortality and respiratory morbidity. Respiratory morbidity includes asthma, chronic obstructive pulmonary disease (COPD), bronchitis and pneumonia. The epidemiological data linking wildfire smoke exposure to cardiovascular mortality and morbidity is mixed, and inconclusive. More studies are needed to define the risk for common and costly clinical cardiovascular outcomes. Susceptible populations include people with respiratory and possibly cardiovascular diseases, middle-aged and older adults, children, pregnant women and the fetus. The increasing frequency of large wildland fires, the expansion of the wildland-urban interface, the area between unoccupied land and human development; and an increasing and aging U.S. population are increasing the number of people at-risk from wildfire smoke, thus highlighting the necessity for broadening stakeholder cooperation to address the health effects of wildfire. While much is known, many questions remain and require further population-based, clinical and occupational health research. Health effects measured over much wider geographical areas and for longer periods time will better define the risk for adverse health outcomes, identify the sensitive populations and assess the influence of social factors on the relationship between exposure and health outcomes. Improving exposure models and access to large clinical databases foreshadow improved risk analysis facilitating more effective risk management. Fuel and smoke management remains an important component for protecting population health. Improved smoke forecasting and translation of environmental health science into communication of actionable information for use by public health officials, healthcare professionals and the public is needed to motivate behaviors that lower exposure and protect public health, particularly among those at high risk.
Keywords: Air pollution; Health effects; Particulate matter, PM(2.5); Smoke; Wildfire emissions.
Published by Elsevier B.V.
Conflict of interest statement
The author declares no competing financial interest.
Figures

References
-
- Bladon KD, Emelko MB, Silins U, Stone M, 2014. Wildfire and the future of water supply. Environ Sci. Technol 48, 8936–43. - PubMed
-
- Chuang HC, Ho KF, Lin LY, Chang TY, Hong GB, Ma CM, Liu IJ, Chuang KJ, 2017. Long-term indoor air conditioner filtration and cardiovascular health: A randomized crossover intervention study. Environ. Int 106, 91–96. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
