

"Hypothyroidism screening during first trimester of pregnancy"
- PMID: 29273014
- PMCID: PMC5741893
- DOI: 10.1186/s12884-017-1624-x
"Hypothyroidism screening during first trimester of pregnancy"
Abstract
Background: Subclinical hypothyroidism is defined as an elevated thyroid-stimulating hormone level with a normal thyroxin level without signs or symptoms of hypothyroidism. Although it is well accepted that overt hypothyroidism has a deleterious impact on pregnancy, recent studies indicate that subclinical hypothyroidism may affect maternal and fetal health. Studies suggest an association between miscarriage and preterm delivery in euthyroid women positive for anti-peroxidase antibodies and/or anti-thyroglobulin antibodies. A proposal of a new set-point to diagnose SCH was recently published. The aim of this research was to determine the optimal thyroid-stimulating hormone cut-off point to screen for subclinical hypothyroidism in the first trimester of gestation in a population of our clinical area and to determine the diagnostic value of this screening test for detecting anti-thyroid peroxidase antibodies.
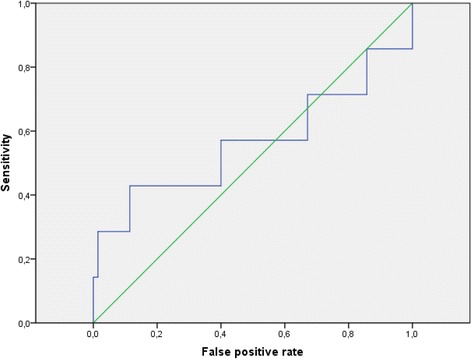
Methods: This cross-sectional study determines the cutoff point for SCH screening and evaluates its usefulness to detect TPO Ab using the Receiver Operating Characteristics (ROC) curve. Prevalence of SCH was calculated using as cut-off 2.5 mIU/L, 4 mIU/L, and our TSH 97.5th percentile. The ability to detect positive anti-thyroglobulin antibodies (TG Ab) and anti-thyroid peroxidase antibodies (TPO Ab) in patients with levels of TSH >97.5th percentile was determined by ROC curves.
Results: The mean, range and standard deviation of TSH was 2.15 ± 1.34 mIU/L (range 0.03-8.82); FT4 was 1.18 ± 0.13 ng/dL (range 0.94-1.3); TG Ab was 89.87 ± 413.56 IU/mL (range 0.10-4000); and TPO Ab was 21.61 ± 46.27 IU/mL(range 0.10-412.4). The ROC. analysis of the ability of the TSH level to predict the presence of positive TPO Ab found an AUC of 0.563.
Conclusion: In our population, the TSH cutoff value for gestational SCH screening is 4.7 mIU/L. Using the SEGO recommended 2.5 mIU/L TSH cut-off point, the prevalence of SCH is 37%. Applying the ATA 2017 recommended cutoff point of 4 mIU/L, the prevalence of SCH is 9.6%. Finally, when the cut-off of 4.7 mIU/L (our 97.5th centile) was used, the SCH prevalence is 5%. TSH levels in the first trimester of pregnancy are not useful to detect TPO Ab.
Keywords: Hypothyroidism; Maternal serum screening tests; Pregnancy complications, diagnosis; Pregnancy trimester, first; Thyroid function tests; Thyrotropin.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the Research Ethics Committee of the University Hospital of Puerto Real, Bahia de Cádiz, La Janda, and Campo de Gibraltar. A written informed consent was obtained from all the participants in the study at enrolment.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Similar articles
-
Maternal thyroid parameters in pregnant women with different ethnic backgrounds: Do ethnicity-specific reference ranges improve the diagnosis of subclinical hypothyroidism?Clin Endocrinol (Oxf). 2017 Jun;86(6):830-836. doi: 10.1111/cen.13340. Epub 2017 Apr 24. Clin Endocrinol (Oxf). 2017. PMID: 28346766
-
[Comparison of the effect of different diagnostic criteria of subclinical hypothyroidism and positive TPO-Ab on pregnancy outcomes].Zhonghua Fu Chan Ke Za Zhi. 2014 Nov;49(11):824-8. Zhonghua Fu Chan Ke Za Zhi. 2014. PMID: 25603906 Chinese.
-
Prevalence of abnormal thyroid stimulating hormone and thyroid peroxidase antibody-positive results in a population of pregnant women in the Samara region of the Russian Federation.Clin Chem Lab Med. 2005;43(11):1223-6. doi: 10.1515/CCLM.2005.212. Clin Chem Lab Med. 2005. PMID: 16232090
-
Hypothyroidism in pregnancy.Lancet Diabetes Endocrinol. 2013 Nov;1(3):228-37. doi: 10.1016/S2213-8587(13)70109-8. Epub 2013 Oct 18. Lancet Diabetes Endocrinol. 2013. PMID: 24622371 Review.
-
Clinical controversies in screening women for thyroid disorders during pregnancy.J Midwifery Womens Health. 2006 May-Jun;51(3):152-8. doi: 10.1016/j.jmwh.2005.11.007. J Midwifery Womens Health. 2006. PMID: 16647667 Review.
Cited by
-
Cluster Analysis: A New Approach for Identification of Underlying Risk Factors and Demographic Features of First Trimester Pregnancy Women.J Clin Med. 2020 Jul 15;9(7):2247. doi: 10.3390/jcm9072247. J Clin Med. 2020. PMID: 32679845 Free PMC article.
-
Thyroid-Stimulating Hormone Values in Pregnancy: Cutoff Controversy Continues?J Obstet Gynaecol India. 2019 Oct;69(5):389-394. doi: 10.1007/s13224-019-01272-w. Epub 2019 Sep 13. J Obstet Gynaecol India. 2019. PMID: 31598039 Free PMC article.
-
A Bayesian model to estimate the cutoff value of TSH for management of preterm birth.PLoS One. 2023 Mar 29;18(3):e0283503. doi: 10.1371/journal.pone.0283503. eCollection 2023. PLoS One. 2023. PMID: 36989309 Free PMC article.
-
Thyroid Hormones in Early Pregnancy and Birth Weight: A Retrospective Study.Biomedicines. 2025 Feb 21;13(3):542. doi: 10.3390/biomedicines13030542. Biomedicines. 2025. PMID: 40149520 Free PMC article.
-
Reference Levels for TSH in Iodine-Sufficient Low-Risk Pregnant Women.J Obstet Gynaecol India. 2021 Dec;71(6):596-599. doi: 10.1007/s13224-021-01477-y. Epub 2021 Apr 2. J Obstet Gynaecol India. 2021. PMID: 34898897 Free PMC article.
References
-
- Haddow JE, Palomaki GE, Allan WC, Williams JR, Knight GJ, Gagnon J, O’Heir CE, Mitchell ML, Hermos RJ, Waisbren SE, Faix JD, Klein RZ. Maternal thyroid deficiency during pregnancy and subsequent neuropsychological development of the child. N Engl J Med. 1999;341:549–555. doi: 10.1056/NEJM199908193410801. - DOI - PubMed
-
- Stagnaro-Green A, Abalovich M, Alexander E, Azizi F, Mestman J, Negro R, Nixon A, Pearce EN, Soldin OP, Sullivan S. Wiersinga W; American Thyroid Association taskforce on thyroid disease during pregnancy and postpartum. Guidelines of the American Thyroid Association for the diagnosis and management of thyroid disease during pregnancy and postpartum. Thyroid. 2011;21:1081–1125. doi: 10.1089/thy.2011.0087. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
