

Cost effectiveness of neoadjuvant chemotherapy followed by interval cytoreductive surgery versus primary cytoreductive surgery for patients with advanced stage ovarian cancer during the initial treatment phase
- PMID: 29273308
- PMCID: PMC6002777
- DOI: 10.1016/j.ygyno.2017.12.015
Cost effectiveness of neoadjuvant chemotherapy followed by interval cytoreductive surgery versus primary cytoreductive surgery for patients with advanced stage ovarian cancer during the initial treatment phase
Abstract
Objective: Advanced stage epithelial ovarian cancer (AEOC) can be treated with either neoadjuvant chemotherapy (NACT) or primary cytoreductive surgery (PCS). Although randomized controlled trials show that NACT is non-inferior in overall survival compared to PCS, there may be improvement in short-term morbidity. We sought to investigate the cost-effectiveness of NACT relative to PCS for AEOC from the US Medicare perspective.
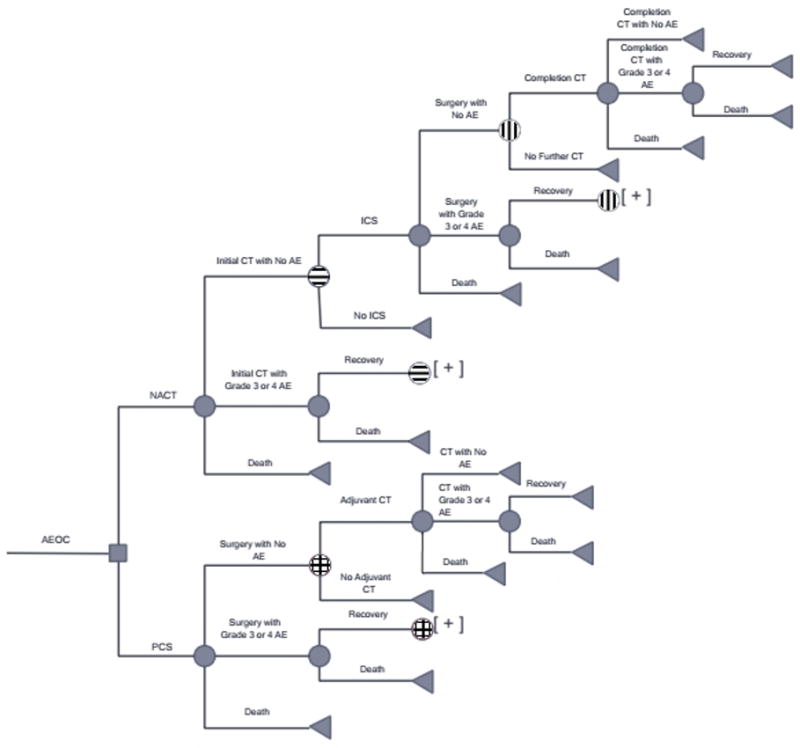
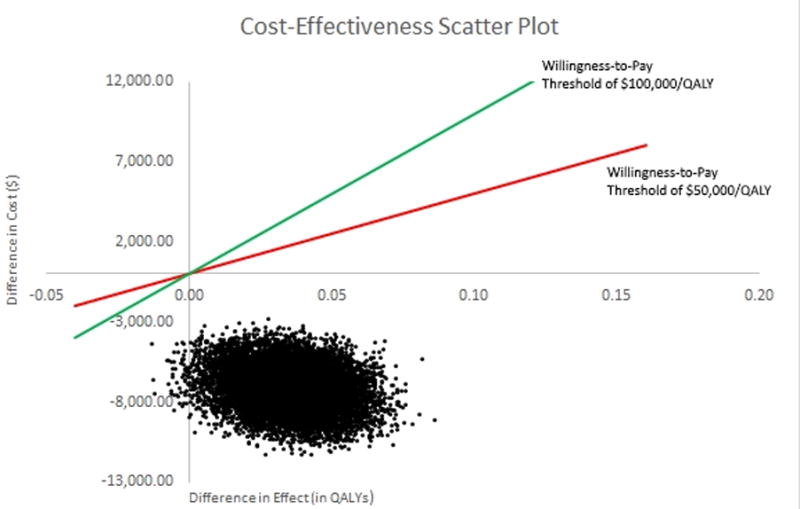
Methods: A cost-effectiveness analysis using a Markov model with a 7-month time horizon comparing (1) 3cycles of NACT with carboplatin and paclitaxel (CT), followed by interval cytoreductive surgery, then 3 additional cycles of CT, or (2) PCS followed by 6cycles of CT. Input parameters included probability of chemotherapy complications, surgical complications, treatment completion, treatment costs, and utilities. Model outcomes included costs, life-years gained, quality-adjusted life-years (QALYs) gained, and incremental cost-effectiveness ratios (ICER), in terms of cost per life-year gained and cost per QALY gained. We accounted for differences in surgical complexity by incorporating the cost of additional procedures and the probability of undergoing those procedures. Probabilistic sensitivity analysis (PSA) was performed via Monte Carlo simulations.
Results: NACT resulted in a savings of $7034 per patient with a 0.035 QALY increase compared to PCS; therefore, NACT dominated PCS in the base case analysis. With PSA, NACT was the dominant strategy more than 99% of the time.
Conclusions: In the short-term, NACT is a cost-effective alternative compared to PCS in women with AEOC. These results may translate to longer term cost-effectiveness; however, data from randomized control trials continues to mature.
Keywords: Cost-effective analysis; Neoadjuvant chemotherapy; Ovarian cancer; Primary cytoreduction.
Copyright © 2017 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016;66(1):7–30. - PubMed
-
- Van der Burg ME, Van Lent M, Buyse M, Kobierska A, Colombo N, Favalli G, Lacave AJ, Nardi M, Renard J, Pecorelli S. The Effect of Debulking Surgery After Induction Chemotherapy on the Prognosis in Advanced Epithelial Ovarian Cancer. N Engl J Med. 1995;332(10):629–634. - PubMed
-
- Vergote I, van Gorp T, Amant F, Leunen K, Neven P, Berteloot P. Timing of debulking surgery in advanced ovarian cancer. Int J Gynecol Cancer. 2008;18(Suppl 1):11–9. - PubMed
-
- Hoskins WJ, McGuire WP, Brady MF, Homesley HD, Greasman WT, Berman M, Ball H, Berek JS. The effect of diameter of largest residual disease on survival after primary cytoreductive surgery in patients with suboptimal residual epithelial ovarian carcinoma. Am J Obstet Gynecol. 1994;170(4) 974-9-80. - PubMed
-
- Hoskins WJ, Bundy BN, Thigpen JT, Omura GA. The influence of cytoreductive surgery on recurrence-free interval and survival in small-volume stage III epithelial ovarian cancer: A gynecologic oncology group study. Gynecol Oncol. 1992;47(2):159–66. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
