

The satisfactory growth and development at 2 years of age of the INTERGROWTH-21st Fetal Growth Standards cohort support its appropriateness for constructing international standards
- PMID: 29273309
- PMCID: PMC5807090
- DOI: 10.1016/j.ajog.2017.11.564
The satisfactory growth and development at 2 years of age of the INTERGROWTH-21st Fetal Growth Standards cohort support its appropriateness for constructing international standards
Abstract
Background: The World Health Organization recommends that human growth should be monitored with the use of international standards. However, in obstetric practice, we continue to monitor fetal growth using numerous local charts or equations that are based on different populations for each body structure. Consistent with World Health Organization recommendations, the INTERGROWTH-21st Project has produced the first set of international standards to date pregnancies; to monitor fetal growth, estimated fetal weight, Doppler measures, and brain structures; to measure uterine growth, maternal nutrition, newborn infant size, and body composition; and to assess the postnatal growth of preterm babies. All these standards are based on the same healthy pregnancy cohort. Recognizing the importance of demonstrating that, postnatally, this cohort still adhered to the World Health Organization prescriptive approach, we followed their growth and development to the key milestone of 2 years of age.
Objective: The purpose of this study was to determine whether the babies in the INTERGROWTH-21st Project maintained optimal growth and development in childhood.
Study design: In the Infant Follow-up Study of the INTERGROWTH-21st Project, we evaluated postnatal growth, nutrition, morbidity, and motor development up to 2 years of age in the children who contributed data to the construction of the international fetal growth, newborn infant size and body composition at birth, and preterm postnatal growth standards. Clinical care, feeding practices, anthropometric measures, and assessment of morbidity were standardized across study sites and documented at 1 and 2 years of age. Weight, length, and head circumference age- and sex-specific z-scores and percentiles and motor development milestones were estimated with the use of the World Health Organization Child Growth Standards and World Health Organization milestone distributions, respectively. For the preterm infants, corrected age was used. Variance components analysis was used to estimate the percentage variability among individuals within a study site compared with that among study sites.
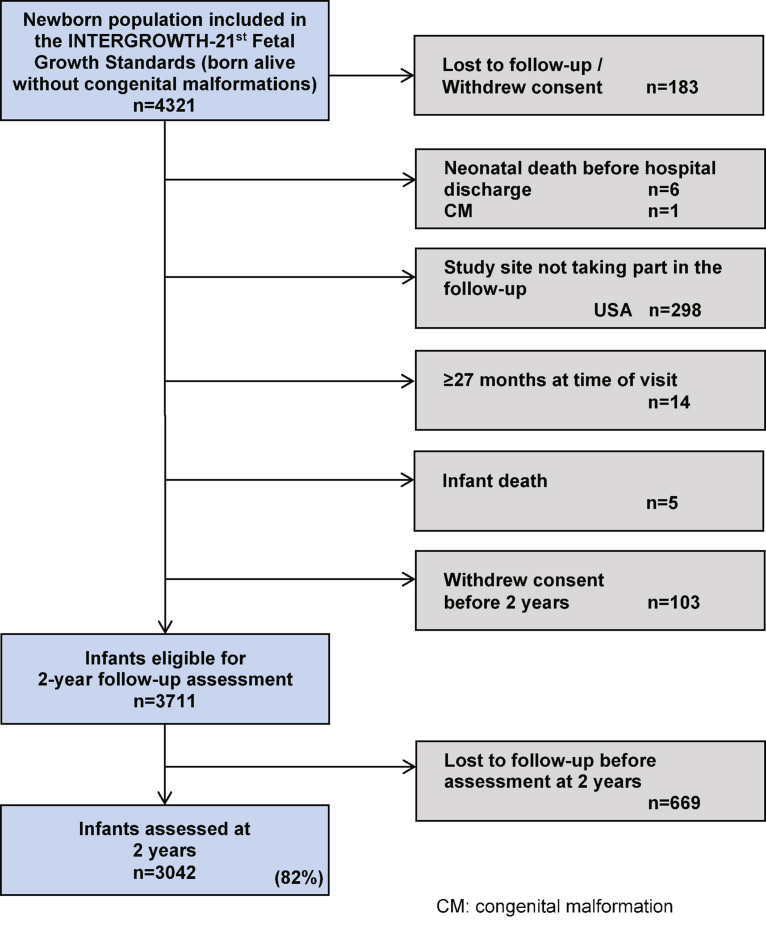
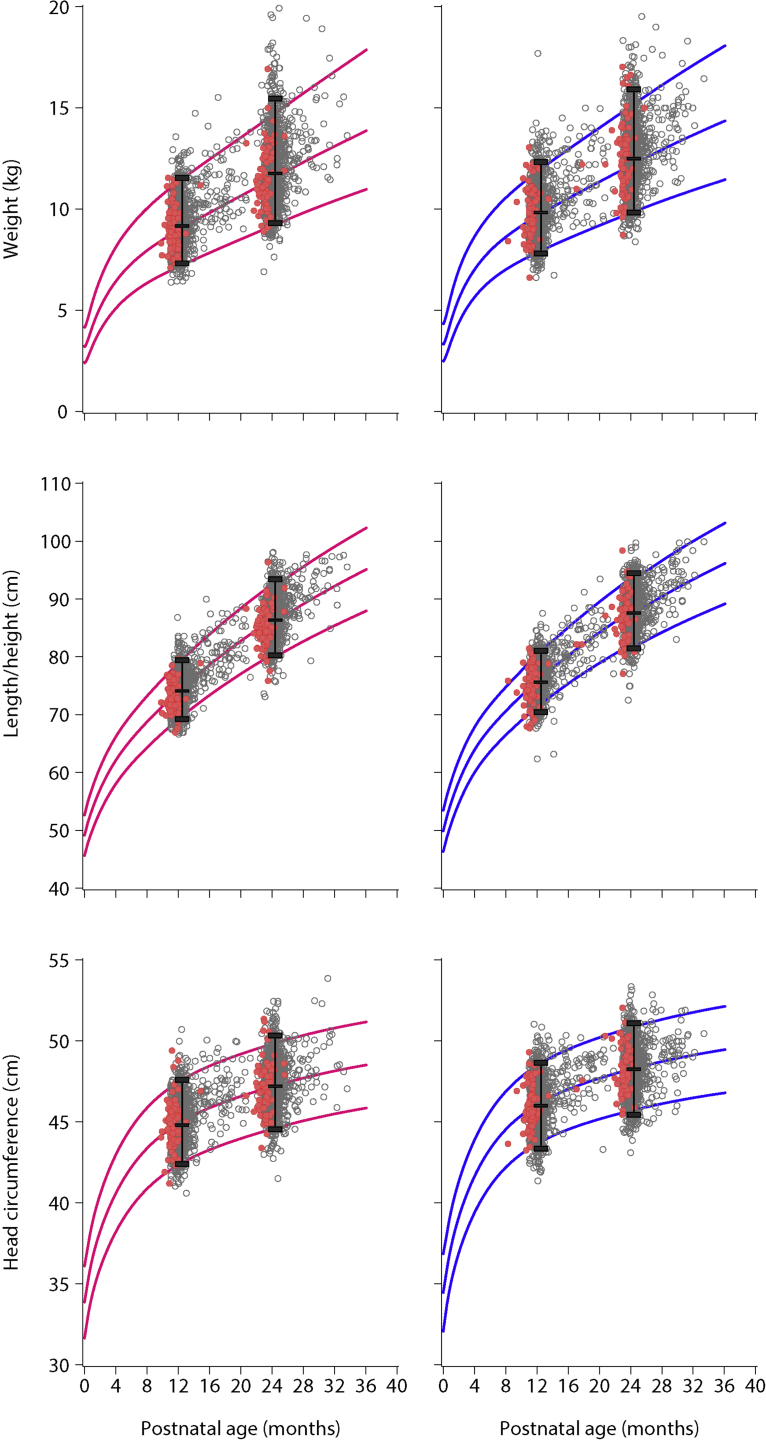
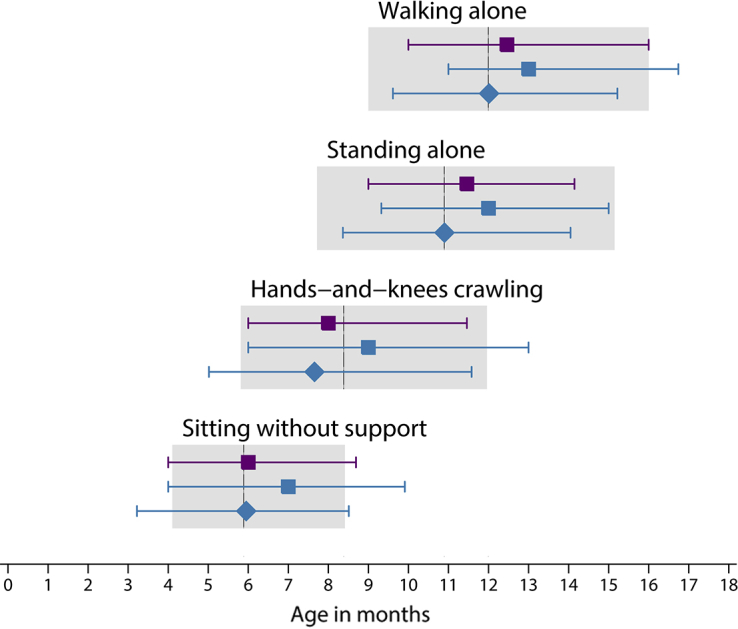
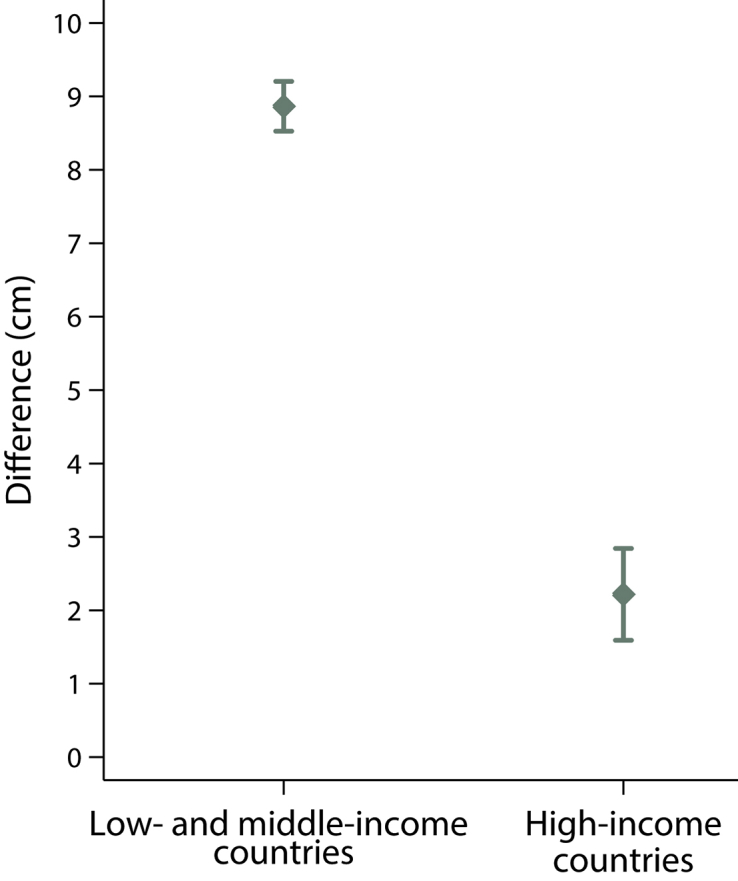
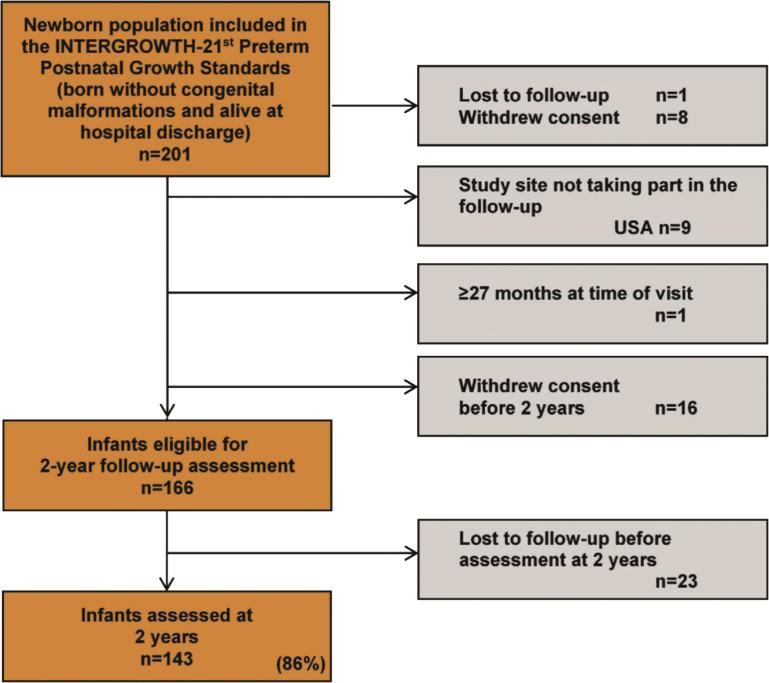
Results: There were 3711 eligible singleton live births; 3042 children (82%) were evaluated at 2 years of age. There were no substantive differences between the included group and the lost-to-follow up group. Infant mortality rate was 3 per 1000; neonatal mortality rate was 1.6 per 1000. At the 2-year visit, the children included in the INTERGROWTH-21st Fetal Growth Standards were at the 49th percentile for length, 50th percentile for head circumference, and 58th percentile for weight of the World Health Organization Child Growth Standards. Similar results were seen for the preterm subgroup that was included in the INTERGROWTH-21st Preterm Postnatal Growth Standards. The cohort overlapped between the 3rd and 97th percentiles of the World Health Organization motor development milestones. We estimated that the variance among study sites explains only 5.5% of the total variability in the length of the children between birth and 2 years of age, although the variance among individuals within a study site explains 42.9% (ie, 8 times the amount explained by the variation among sites). An increase of 8.9 cm in adult height over mean parental height is estimated to occur in the cohort from low-middle income countries, provided that children continue to have adequate health, environmental, and nutritional conditions.
Conclusion: The cohort enrolled in the INTERGROWTH-21st standards remained healthy with adequate growth and motor development up to 2 years of age, which supports its appropriateness for the construction of international fetal and preterm postnatal growth standards.
Keywords: INTERGROWTH-21(st) fetal growth standards; development; postnatal growth.
Copyright © 2017 The Author(s). Published by Elsevier Inc. All rights reserved.
Figures
References
-
- World Health Organization. Screening, assessment and management of neonates and infants with complications associated with Zika virus exposure in utero: Interim guidance update. 2016; WHO/ZIKV/MOC/16.3 Rev.2. Available at: http://apps.who.int/iris/bitstream/10665/204475/1/WHO_ZIKV_MOC_16.3_eng.pdf. Accessed August 30, 2016.
-
- Centers for Disease Control and Prevention. Congenital microcephaly case definitions. 2016. Available at: http://www.cdc.gov/zika/public-health-partners/microcephaly-case-definit.... Accessed November 30, 2016.
-
- Villar J., Papageorghiou A.T., Pang R. Monitoring human growth and development: a continuum from the womb to the classroom. Am J Obstet Gynecol. 2015;213:494–499. - PubMed
-
- Villar J, Giuliani F, Barros FC, et al. Monitoring the postnatal growth of preterm infants: a paradigm change. Pediatrics 2018 Jan 4. pii: e20172467. https://doi.org/10.1542/peds.2017-2467. [Epub ahead of print]. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
