

Effectiveness of WHO's pragmatic screening algorithm for child contacts of tuberculosis cases in resource-constrained settings: a prospective cohort study in Uganda
- PMID: 29273539
- PMCID: PMC5876110
- DOI: 10.1016/S2213-2600(17)30497-6
Effectiveness of WHO's pragmatic screening algorithm for child contacts of tuberculosis cases in resource-constrained settings: a prospective cohort study in Uganda
Abstract
Background: Tuberculosis is a leading cause of global childhood mortality; however, interventions to detect undiagnosed tuberculosis in children are underused. Child contact tracing has been widely recommended but poorly implemented in resource-constrained settings. WHO has proposed a pragmatic screening approach for managing child contacts. We assessed the effectiveness of this screening approach and alternative symptom-based algorithms in identifying secondary tuberculosis in a prospectively followed cohort of Ugandan child contacts.
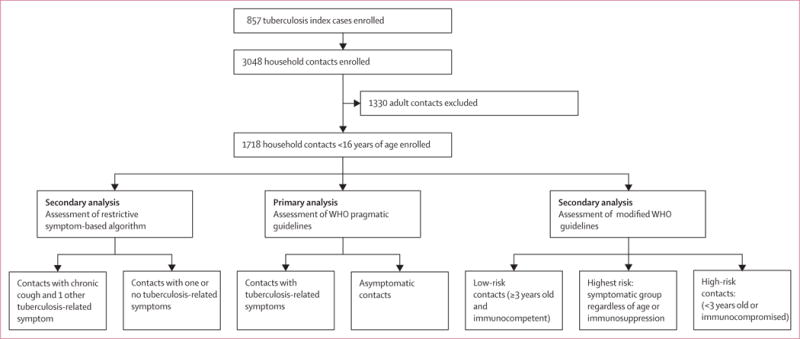
Methods: We identified index patients aged at least 18 years with microbiologically confirmed pulmonary tuberculosis at Old Mulago Hospital (Kampala, Uganda) between Oct 1, 1995, and Dec 31, 2008. Households of index patients were visited by fieldworkers within 2 weeks of diagnosis. Coprevalent and incident tuberculosis were assessed in household contacts through clinical, radiographical, and microbiological examinations for 2 years. Disease rates were compared among children younger than 16 years with and without symptoms included in the WHO pragmatic guideline (presence of haemoptysis, fever, chronic cough, weight loss, night sweats, and poor appetite). Symptoms could be of any duration, except cough (>21 days) and fever (>14 days). A modified WHO decision-tree designed to detect high-risk asymptomatic child contacts was also assessed, in which all asymptomatic contacts were classified as high risk (children younger than 3 years or immunocompromised [HIV-infected]) or low risk (aged 3 years or older and immunocompetent [HIV-negative]). We also assessed a more restrictive algorithm (ie, assessing only children with presence of chronic cough and one other tuberculosis-related symptom).
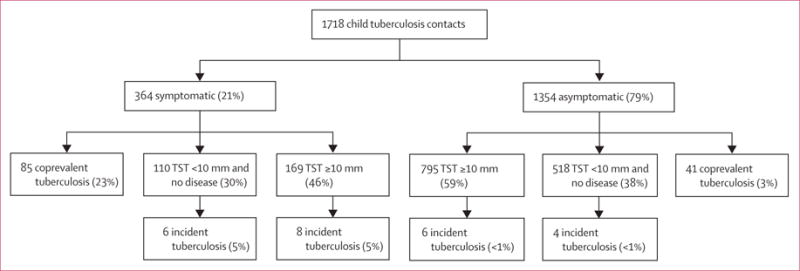
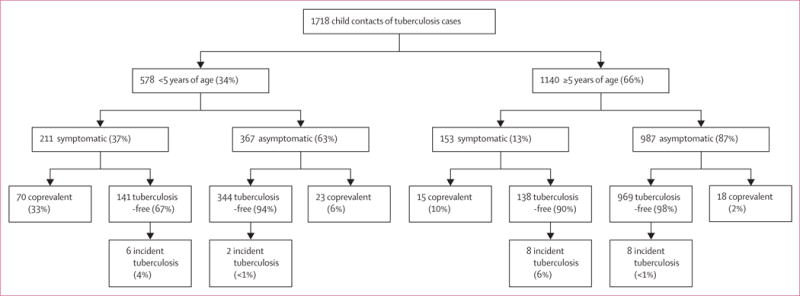
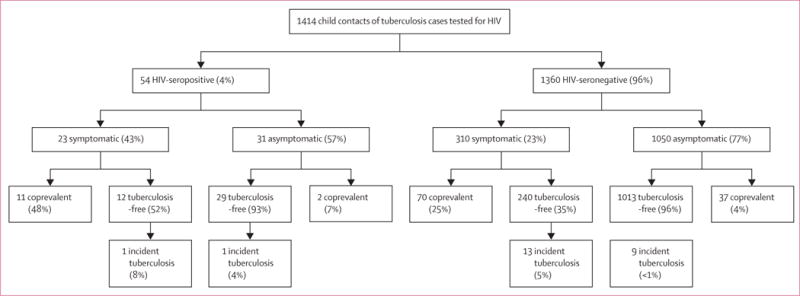
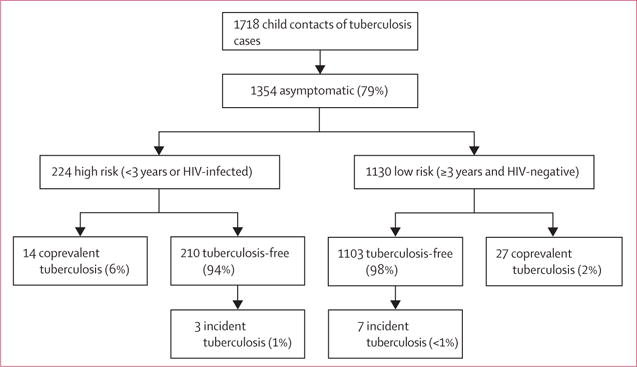
Findings: Of 1718 household child contacts, 126 (7%) had coprevalent tuberculosis and 24 (1%) developed incident tuberculosis, diagnosed over the 2-year study period. Of these 150 cases of tuberculosis, 95 (63%) were microbiologically confirmed with a positive sputum culture. Using the WHO approach, 364 (21%) of 1718 child contacts had at least one tuberculosis-related symptom and 85 (23%) were identified as having coprevalent tuberculosis, 67% of all coprevalent cases detected (diagnostic odds ratio 9·8, 95% CI 6·8-14·5; p<0·0001). 1354 (79%) of 1718 child contacts had no symptoms, of whom 41 (3%) had coprevalent tuberculosis. The WHO approach was effective in contacts younger than 5 years: 70 (33%) of 211 symptomatic contacts had coprevalent disease compared with 23 (6%) of 367 asymptomatic contacts (p<0·0001). This approach was also effective in contacts aged 5 years and older: 15 (10%) of 153 symptomatic contacts had coprevalent disease compared with 18 (2%) of 987 asymptomatic contacts (p<0·0001). More coprevalent disease was detected in child contacts recommended for screening when the study population was restricted by HIV-serostatus (11 [48%] of 23 symptomatic HIV-seropositive child contacts vs two [7%] of 31 asymptomatic HIV-seropositive child contacts) or to only culture-confirmed cases (47 [13%] culture confirmed cases of 364 symptomatic child contacts vs 29 [2%] culture confirmed cases of 1354 asymptomatic child contacts). In the modified algorithm, high-risk asymptomatic child contacts were at increased risk for coprevalent disease versus low-risk asymptomatic contacts (14 [6%] of 224 vs 27 [2%] of 1130; p=0·0021). The presence of tuberculosis infection did not predict incident disease in either symptomatic or asymptomatic child contacts: in symptomatic contacts, eight (5%) of 169 infected contacts and six (5%) of 111 uninfected contacts developed incident tuberculosis (p=0·80). Among asymptomatic contacts, incident tuberculosis occurred in six (<1%) of 795 contacts infected at baseline versus four (<1%) of 518 contacts uninfected at baseline, respectively (p=1·00).
Interpretation: WHO's pragmatic, symptom-based algorithm was an effective case-finding tool, especially in children younger than 5 years. A modified decision-tree identified 6% of asymptomatic child contacts at high risk for subclinical disease. Increasing the feasibility of child-contact tracing using these approaches should be encouraged to decrease tuberculosis-related paediatric mortality in high-burden settings, but this should be partnered with increasing access to microbiological point-of-care testing.
Funding: National Institutes of Health, Tuberculosis Research Unit, AIDS International Training and Research Program of the Fogarty International Center, and the Center for AIDS Research.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Conflict of interest statement
CMS and WHB report grants from the National Institutes of Health. All other authors declare no competing interests.
Figures
Comment in
-
Symptom-based screening of children with household tuberculosis contact.Lancet Respir Med. 2018 Apr;6(4):235-237. doi: 10.1016/S2213-2600(17)30496-4. Epub 2017 Dec 19. Lancet Respir Med. 2018. PMID: 29273537 No abstract available.
Similar articles
-
Screening tests for active pulmonary tuberculosis in children.Cochrane Database Syst Rev. 2021 Jun 28;6(6):CD013693. doi: 10.1002/14651858.CD013693.pub2. Cochrane Database Syst Rev. 2021. PMID: 34180536 Free PMC article.
-
Infectiousness of HIV-Seropositive Patients with Tuberculosis in a High-Burden African Setting.Am J Respir Crit Care Med. 2016 Nov 1;194(9):1152-1163. doi: 10.1164/rccm.201511-2146OC. Am J Respir Crit Care Med. 2016. PMID: 27181053 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
A refined symptom-based approach to diagnose pulmonary tuberculosis in children.Pediatrics. 2006 Nov;118(5):e1350-9. doi: 10.1542/peds.2006-0519. Pediatrics. 2006. PMID: 17079536
-
Screening for Asymptomatic Tuberculosis among Adults with Household Exposure to a Patient with Pulmonary Tuberculosis.medRxiv [Preprint]. 2025 Jan 20:2025.01.20.25320843. doi: 10.1101/2025.01.20.25320843. medRxiv. 2025. PMID: 39974049 Free PMC article. Preprint.
Cited by
-
Scaling up investigation and treatment of household contacts of tuberculosis patients in Brazil: a cost-effectiveness and budget impact analysis.Lancet Reg Health Am. 2022 Jan 10;8:100166. doi: 10.1016/j.lana.2021.100166. eCollection 2022 Apr. Lancet Reg Health Am. 2022. PMID: 36778732 Free PMC article.
-
The Contribution of Chest Radiography to the Clinical Management of Children Exposed to Tuberculosis.Am J Respir Crit Care Med. 2022 Oct 1;206(7):892-900. doi: 10.1164/rccm.202202-0259OC. Am J Respir Crit Care Med. 2022. PMID: 35608549 Free PMC article.
-
Comparison of yield and relative costs of different screening algorithms for tuberculosis in active case-finding: a cross-section study.BMC Infect Dis. 2021 Aug 13;21(1):813. doi: 10.1186/s12879-021-06486-w. BMC Infect Dis. 2021. PMID: 34388976 Free PMC article.
-
Vitamin D Concentrations in Infancy and the Risk of Tuberculosis Disease in Childhood: A Prospective Birth Cohort in Cape Town, South Africa.Clin Infect Dis. 2022 Jun 10;74(11):2036-2043. doi: 10.1093/cid/ciab735. Clin Infect Dis. 2022. PMID: 34436538 Free PMC article.
-
Implementation approaches for leprosy prevention with single-dose rifampicin: A support tool for decision making.PLoS Negl Trop Dis. 2022 Oct 17;16(10):e0010792. doi: 10.1371/journal.pntd.0010792. eCollection 2022 Oct. PLoS Negl Trop Dis. 2022. PMID: 36251696 Free PMC article. Review.
References
-
- Marais BJ, Pai M. New approaches and emerging technologies in the diagnosis of childhood tuberculosis. Paediatr Respir Rev. 2007;8:124–33. - PubMed
-
- Maher D, Chaulet P, Spinaci S, Harries A. Treatment of tuberculosis: guidelines for national programmes. 2nd. Geneva: 1997. For World Health Organization Global tuberculosis programme. WHO/TB/97.220.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
