

Health Insurance and the Use of Peritoneal Dialysis in the United States
- PMID: 29277511
- PMCID: PMC6502758
- DOI: 10.1053/j.ajkd.2017.09.024
Health Insurance and the Use of Peritoneal Dialysis in the United States
Abstract
Background: Many patients in the United States have limited or no health insurance at the time they develop end-stage renal disease (ESRD). We examined whether health insurance limitations affected the likelihood of peritoneal dialysis (PD) use.
Study design: Retrospective cohort analysis of patients from the US Renal Data System initiating dialysis therapy in 2006 through 2012.
Setting & participants: We identified socioeconomically similar groups of patients to examine the association between health insurance and PD use. Patients aged 60 to 64 years with "limited insurance" (defined as having Medicaid or no insurance) at ESRD onset were compared with patients aged 66 to 70 years who were dually eligible for Medicare and Medicaid at ESRD onset.
Predictor: Type of insurance coverage at ESRD onset.
Outcomes: The likelihoods of receiving PD before dialysis month 4, when all patients qualified for Medicare due to ESRD, and of switching to PD therapy following receipt of Medicare.
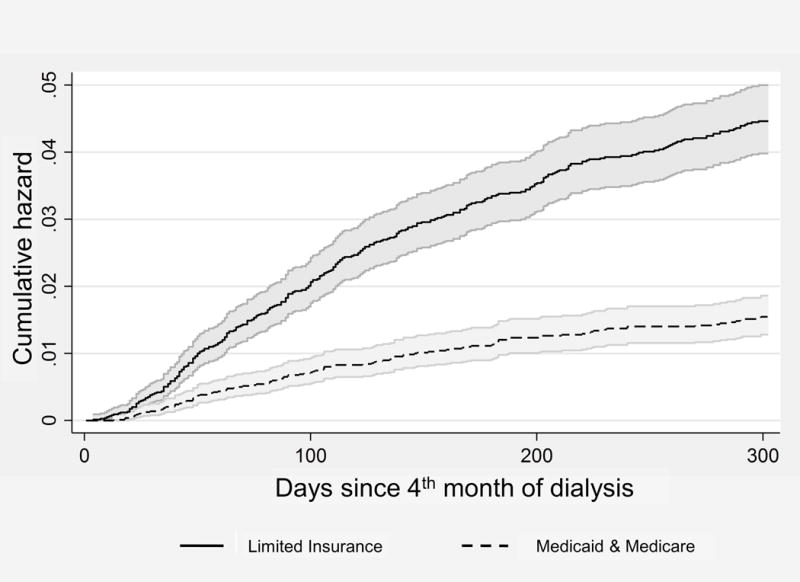
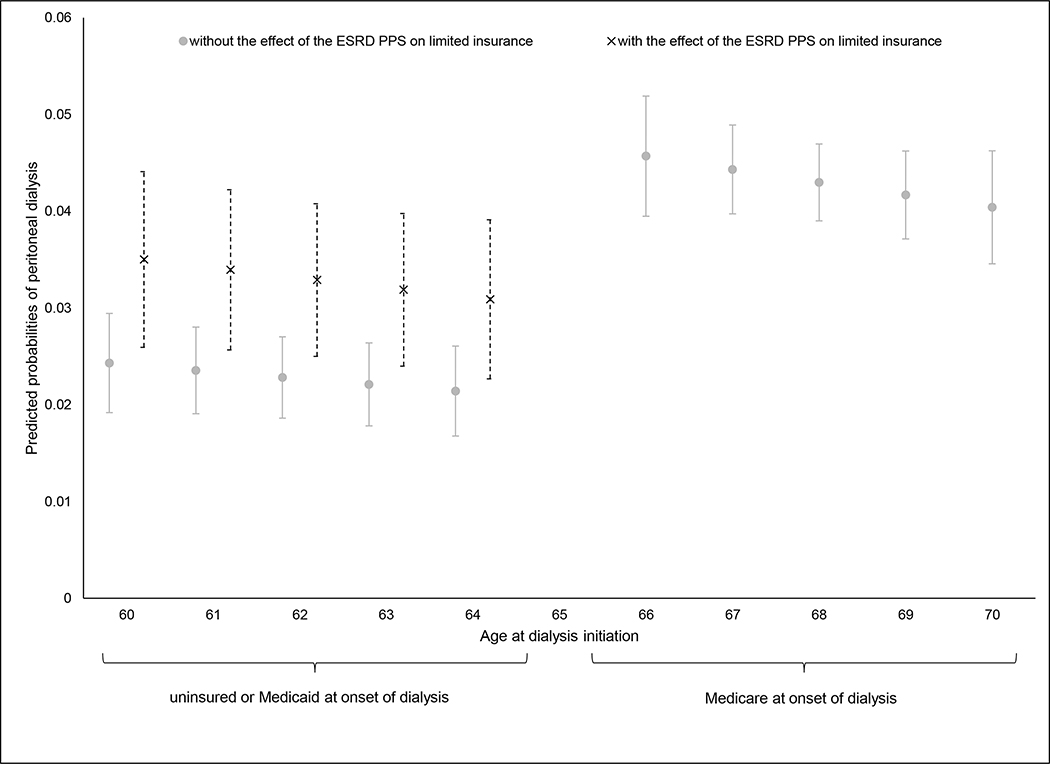
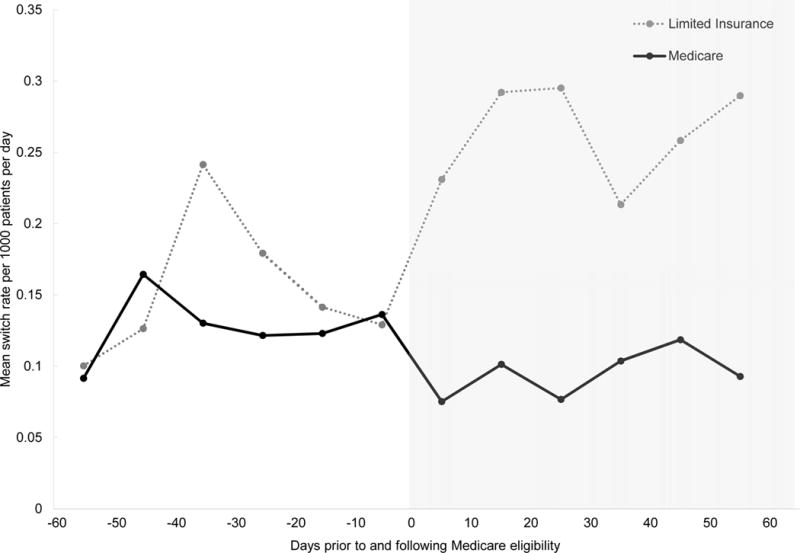
Results: After adjusting for observable patient and geographic differences, patients with limited insurance had an absolute 2.4% (95% CI, 1.1%-3.7%) lower probability of PD use by dialysis month 4 compared with patients with Medicare at ESRD onset. The association between insurance and PD use reversed when patients became Medicare eligible; patients with limited insurance had a 3-fold higher rate of switching to PD therapy between months 4 and 12 of dialysis (HR, 2.9; 95% CI, 1.8-4.6) compared with patients with Medicare at ESRD onset.
Limitations: Because this study was observational, there is a potential for bias from unmeasured patient-level factors.
Conclusions: Despite Medicare's policy of covering patients in the month that they initiate PD therapy, insurance limitations remain a barrier to PD use for many patients. Educating providers about Medicare reimbursement policy and expanding access to pre-ESRD education and training may help overcome these barriers.
Keywords: Health insurance; Medicaid; Medicare; PD use; US Renal Data System (USRDS); dialysis modality; end-stage renal disease (ESRD); health disparities; health economics; hemodialysis (HD); insurance coverage; peritoneal dialysis (PD); renal replacement therapy (RRT).
Copyright © 2017 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Rising Peritoneal Dialysis Tide May Still Leave Some Patients Behind.Am J Kidney Dis. 2018 Apr;71(4):455-457. doi: 10.1053/j.ajkd.2018.01.001. Am J Kidney Dis. 2018. PMID: 29579417 No abstract available.
Similar articles
-
Health Insurance in the First 3 Months of Hemodialysis and Early Vascular Access.Clin J Am Soc Nephrol. 2018 Dec 7;13(12):1866-1875. doi: 10.2215/CJN.06660518. Epub 2018 Nov 1. Clin J Am Soc Nephrol. 2018. PMID: 30385594 Free PMC article.
-
Can dialysis patients be accurately identified using healthcare claims data?Perit Dial Int. 2014 Sep-Oct;34(6):643-51. doi: 10.3747/pdi.2012.00328. Epub 2014 Feb 4. Perit Dial Int. 2014. PMID: 24497600 Free PMC article.
-
The effect of insurance status on use of recombinant erythropoietin therapy among end-stage renal disease patients in three states.Am J Kidney Dis. 1996 Aug;28(2):235-49. doi: 10.1016/s0272-6386(96)90307-8. Am J Kidney Dis. 1996. PMID: 8768919
-
Exploring kidney dialysis costs in the United States: a scoping review.J Med Econ. 2024 Jan-Dec;27(1):618-625. doi: 10.1080/13696998.2024.2342210. Epub 2024 Apr 25. J Med Econ. 2024. PMID: 38605648
-
Assisted Peritoneal Dialysis for Older People with End-Stage Renal Disease: The French and Danish Experience.Perit Dial Int. 2015 Nov;35(6):663-6. doi: 10.3747/pdi.2014.00344. Perit Dial Int. 2015. PMID: 26702010 Free PMC article. Review.
Cited by
-
Home Dialysis in the United States: A Roadmap for Increasing Peritoneal Dialysis Utilization.Am J Kidney Dis. 2020 Mar;75(3):413-416. doi: 10.1053/j.ajkd.2019.10.013. Epub 2020 Jan 17. Am J Kidney Dis. 2020. PMID: 31959369 Free PMC article. No abstract available.
-
Association of Medicaid Expansion With 1-Year Mortality Among Patients With End-Stage Renal Disease.JAMA. 2018 Dec 4;320(21):2242-2250. doi: 10.1001/jama.2018.16504. JAMA. 2018. PMID: 30422251 Free PMC article.
-
Safety-Net Care for Maintenance Dialysis in the United States.J Am Soc Nephrol. 2020 Feb;31(2):424-433. doi: 10.1681/ASN.2019040417. Epub 2019 Dec 19. J Am Soc Nephrol. 2020. PMID: 31857351 Free PMC article.
-
Results of the European EDITH nephrologist survey on factors influencing treatment modality choice for end-stage kidney disease.Nephrol Dial Transplant. 2021 Dec 31;37(1):126-138. doi: 10.1093/ndt/gfaa342. Nephrol Dial Transplant. 2021. PMID: 33486525 Free PMC article.
-
Social determinants of health and chronic kidney disease in United States adults: A cross-sectional study from National Health and Nutrition Examination Survey 2003-2018.Prev Med Rep. 2025 Jun 9;55:103132. doi: 10.1016/j.pmedr.2025.103132. eCollection 2025 Jul. Prev Med Rep. 2025. PMID: 40547890 Free PMC article.
References
-
- National Institutes of Health, National Institutes of Diabetes and Digestive and Kidney Disease, editor. United States Renal Data System. 2016 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States. Bethesda, MD: 2016.
-
- Cook NL, Hicks LS, O’Malley AJ, Keegan T, Guadagnoli E, Landon BE. Access to specialty care and medical services in community health centers. Health affairs (Project Hope) 2007;26:1459–1468. - PubMed
-
- Asplin BR, Rhodes KV, Levy H, et al. Insurance status and access to urgent ambulatory care follow-up appointments. JAMA. 294:1248–1254. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
