

Genomic perturbations reveal distinct regulatory networks in intrahepatic cholangiocarcinoma
- PMID: 29278425
- PMCID: PMC6599967
- DOI: 10.1002/hep.29764
Genomic perturbations reveal distinct regulatory networks in intrahepatic cholangiocarcinoma
Abstract
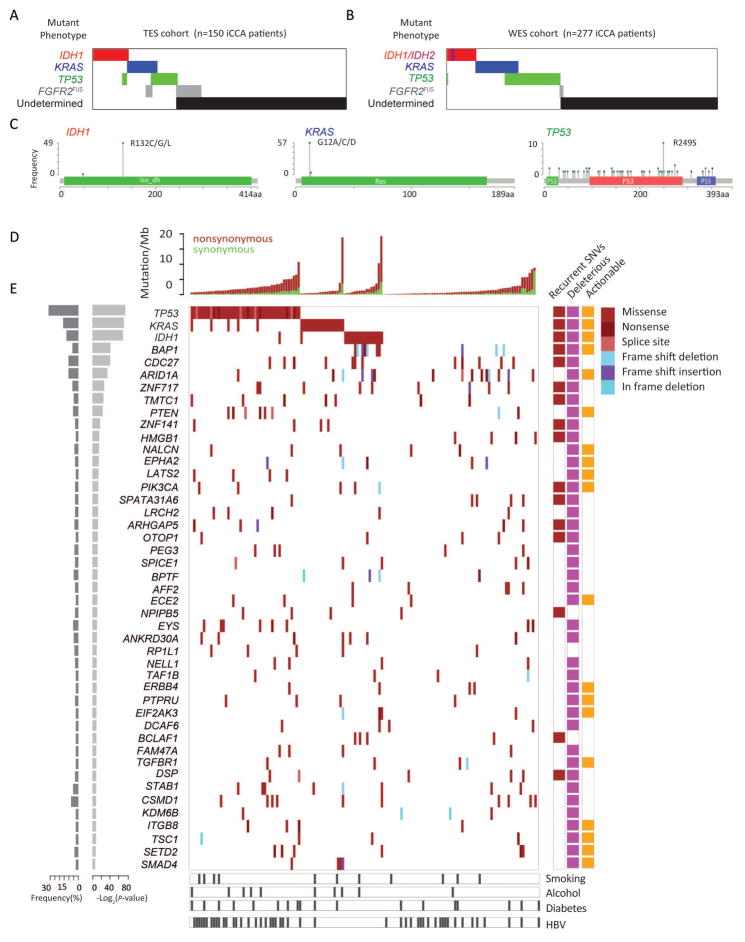
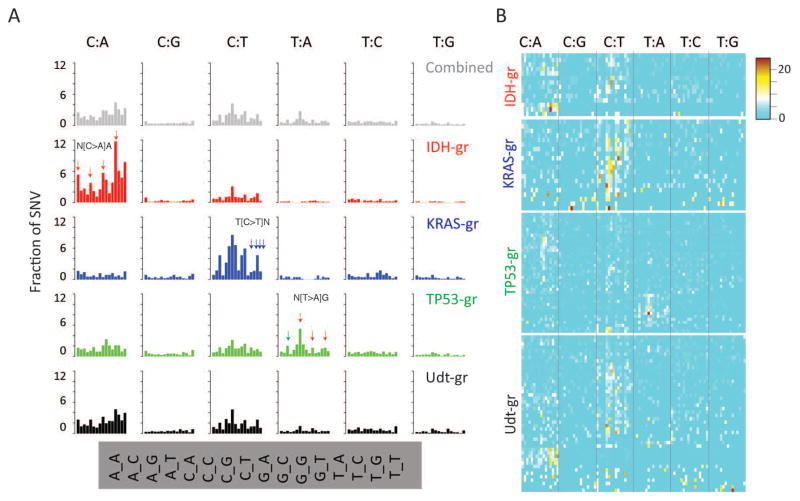
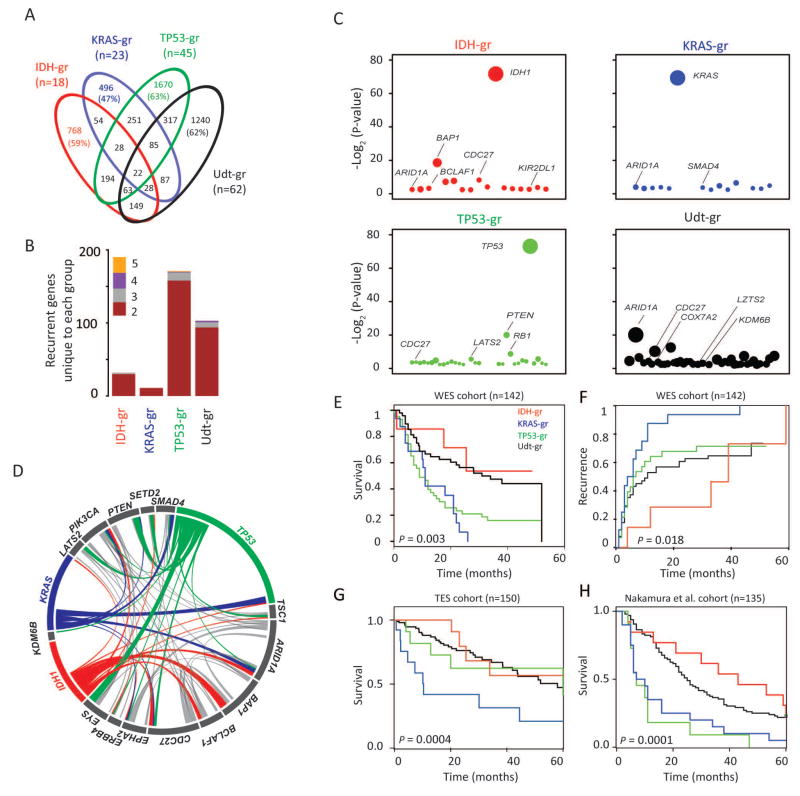
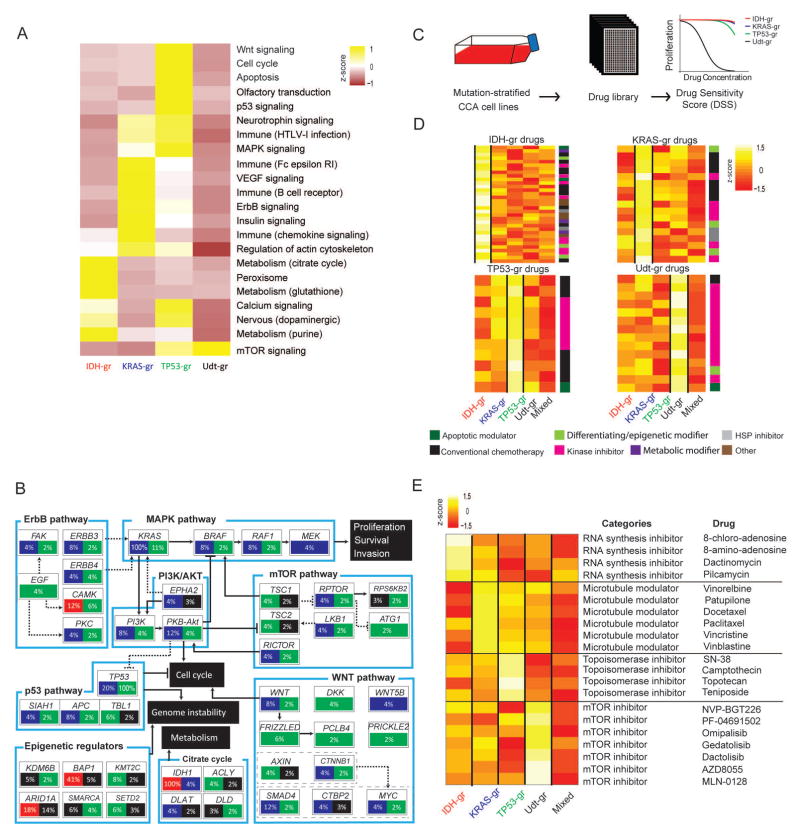
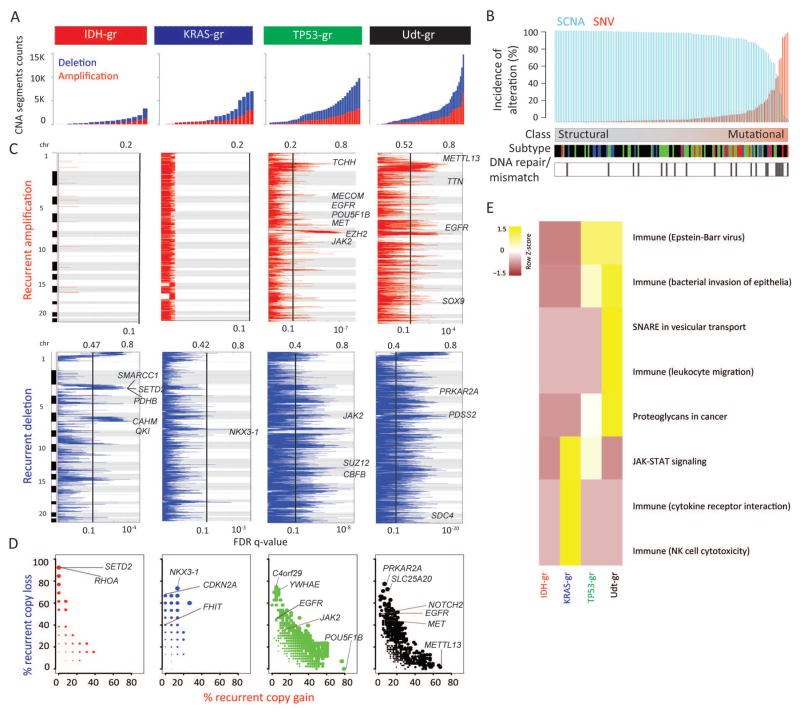
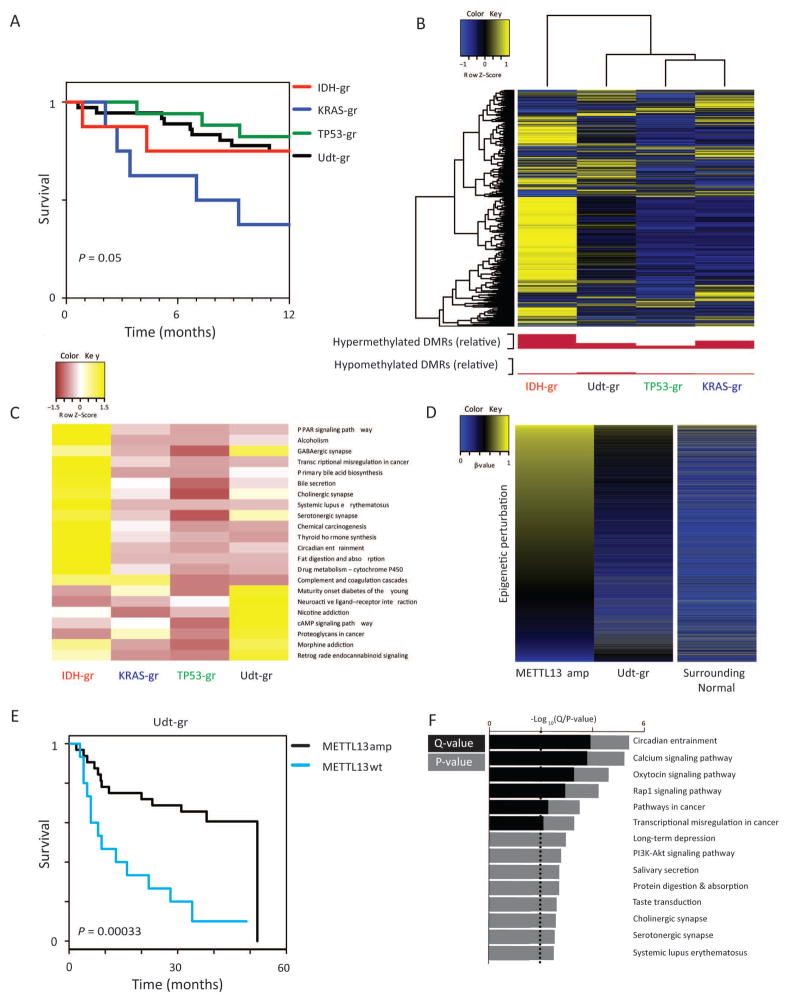
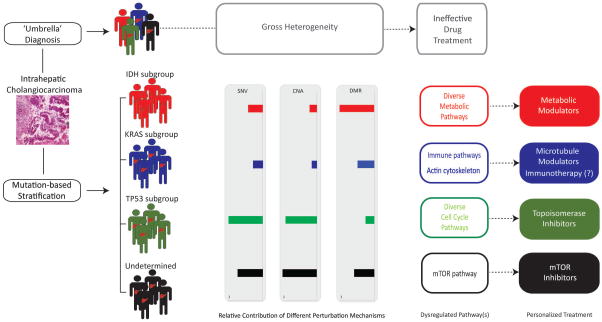
Intrahepatic cholangiocarcinoma remains a highly heterogeneous malignancy that has eluded effective patient stratification to date. The extent to which such heterogeneity can be influenced by individual driver mutations remains to be evaluated. Here, we analyzed genomic (whole-exome sequencing, targeted exome sequencing) and epigenomic data from 496 patients and used the three most recurrently mutated genes to stratify patients (IDH, KRAS, TP53, "undetermined"). Using this molecular dissection approach, each subgroup was determined to possess unique mutational signature preferences, comutation profiles, and enriched pathways. High-throughput drug repositioning in seven patient-matched cell lines, chosen to reflect the genetic alterations specific for each patient group, confirmed in silico predictions of subgroup-specific vulnerabilities linked to enriched pathways. Intriguingly, patients lacking all three mutations ("undetermined") harbored the most extensive structural alterations, while isocitrate dehydrogenase mutant tumors displayed the most extensive DNA methylome dysregulation, consistent with previous findings.
Conclusion: Stratification of intrahepatic cholangiocarcinoma patients based on occurrence of mutations in three classifier genes (IDH, KRAS, TP53) revealed unique oncogenic programs (mutational, structural, epimutational) that influence pharmacologic response in drug repositioning protocols; this genome dissection approach highlights the potential of individual mutations to induce extensive molecular heterogeneity and could facilitate advancement of therapeutic response in this dismal disease. (Hepatology 2018).
© 2017 by the American Association for the Study of Liver Diseases.
Figures
Comment in
-
Toward personalized medicine for intrahepatic cholangiocarcinoma: Pharmacogenomic stratification of patients.Hepatology. 2018 Sep;68(3):811-814. doi: 10.1002/hep.29830. Epub 2018 May 14. Hepatology. 2018. PMID: 29394502 No abstract available.
References
-
- Banales JM, Cardinale V, Carpino G, Marzioni M, Andersen JB, Invernizzi P, Lind GE, et al. Expert consensus document: Cholangiocarcinoma: current knowledge and future perspectives consensus statement from the European Network for the Study of Cholangiocarcinoma (ENS-CCA) Nat Rev Gastroenterol Hepatol. 2016;13:261–280. - PubMed
-
- Claessen MM, Vleggaar FP, Tytgat KM, Siersema PD, van Buuren HR. High lifetime risk of cancer in primary sclerosing cholangitis. J Hepatol. 2009;50:158–164. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
