

Treatment of severe skin and soft tissue infections: a review
- PMID: 29278528
- PMCID: PMC6200137
- DOI: 10.1097/QCO.0000000000000431
Treatment of severe skin and soft tissue infections: a review
Abstract
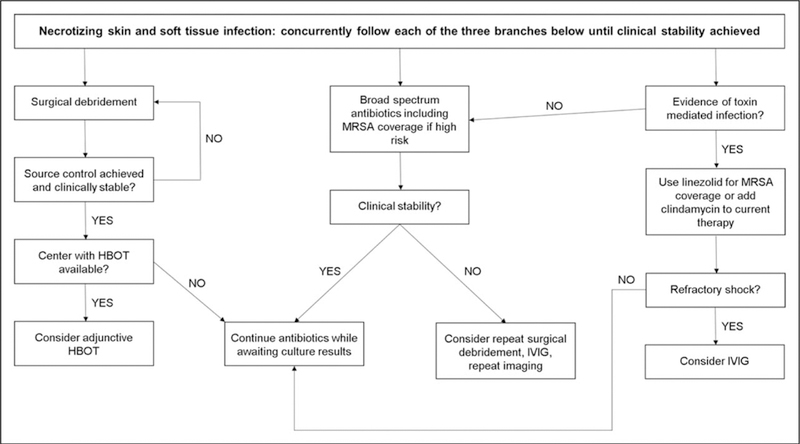
Purpose of review: To review the salient features of the management of severe skin and soft tissue infections (SSTIs), including toxic shock syndrome, myonecrosis/gas gangrene, and necrotizing fasciitis.
Recent findings: For severe SSTIs, intensive care, source control, and broad-spectrum antimicrobials are required for the initial phase of illness. There is an increasing focus on the utility of rapid diagnostic tests to help in selection and de-escalation of antimicrobials for SSTIs. In addition, clinical prediction scores have shown promise in helping predict patients who do not require antimicrobials directed against methicillin-resistant Staphylococcus aureus. Immune status has been shown to be important in clinical outcomes of some, but not all types of SSTIs. The debate for benefits of intravenous immunoglobulin continues to be waged in the recent literature.
Summary: Severe SSTIs are common and their management complex due to regional variation in predominant pathogens and antimicrobial resistance patterns, as well variations in host immune responses. Unique aspects of care for severe SSTIs are discussed including the role of surgical consultation and source control. The unique features of SSTIs in immunocompromised hosts are also described.
Conflict of interest statement
Conflicts of interest
The work was performed at Barnes-Jewish Hospital, St. Louis, Missouri.
There are no conflicts of interest.
Figures

Similar articles
-
Diagnosis and management of skin and soft tissue infections in the intensive care unit: a review.Intensive Care Med. 2016 Dec;42(12):1899-1911. doi: 10.1007/s00134-016-4576-0. Epub 2016 Oct 3. Intensive Care Med. 2016. PMID: 27699456 Free PMC article. Review.
-
Severe Skin and Soft-Tissue Infections.Semin Respir Crit Care Med. 2022 Feb;43(1):3-9. doi: 10.1055/s-0041-1740974. Epub 2022 Feb 16. Semin Respir Crit Care Med. 2022. PMID: 35172354 Review.
-
[Skin and soft tissue infections (SSTIs)].Rozhl Chir. 2016;95(4):141-6. Rozhl Chir. 2016. PMID: 27226266 Review. Czech.
-
Study to evaluate the role of severity stratification of skin and soft tissue infections (SSTIs) in formulating treatment strategies and predicting poor prognostic factors.Int J Surg. 2014;12(2):125-33. doi: 10.1016/j.ijsu.2013.11.014. Epub 2013 Dec 6. Int J Surg. 2014. PMID: 24316391
-
Management of skin and soft-tissue infections at a community teaching hospital using a severity-of-illness tool.J Antimicrob Chemother. 2016 Nov;71(11):3268-3275. doi: 10.1093/jac/dkw263. Epub 2016 Aug 3. J Antimicrob Chemother. 2016. PMID: 27494908
Cited by
-
Evaluation of Linezolid Pharmacokinetics in Critically Ill Obese Patients with Severe Skin and Soft Tissue Infections.Antimicrob Agents Chemother. 2021 Jan 20;65(2):e01619-20. doi: 10.1128/AAC.01619-20. Print 2021 Jan 20. Antimicrob Agents Chemother. 2021. PMID: 33257446 Free PMC article.
-
Cervicofacial Infections Caused by Staphylococcus aureus.Ann Maxillofac Surg. 2019 Jul-Dec;9(2):459-464. doi: 10.4103/ams.ams_226_18. Ann Maxillofac Surg. 2019. PMID: 31909036 Free PMC article.
-
Dihydrothiazolo ring-fused 2-pyridone antimicrobial compounds treat Streptococcus pyogenes skin and soft tissue infection.Sci Adv. 2024 Aug 2;10(31):eadn7979. doi: 10.1126/sciadv.adn7979. Epub 2024 Aug 2. Sci Adv. 2024. PMID: 39093975 Free PMC article.
-
Current approach to skin and soft tissue infections. Thinking about continuity of care.Rev Esp Quimioter. 2023 Nov;36 Suppl 1(Suppl 1):37-45. doi: 10.37201/req/s01.10.2023. Epub 2023 Nov 24. Rev Esp Quimioter. 2023. PMID: 37997870 Free PMC article. Review.
-
Dihydrothiazolo ring-fused 2-pyridone antimicrobial compounds treat Streptococcus pyogenes skin and soft tissue infection.bioRxiv [Preprint]. 2024 Jan 3:2024.01.02.573960. doi: 10.1101/2024.01.02.573960. bioRxiv. 2024. Update in: Sci Adv. 2024 Aug 2;10(31):eadn7979. doi: 10.1126/sciadv.adn7979. PMID: 38260261 Free PMC article. Updated. Preprint.
References
-
- Hersh AL, Chambers HF, Maselli JH, Gonzales R. National trends in ambulatory visits and antibiotic prescribing for skin and soft-tissue infections. Arch Intern Med 2008; 168:1585–1591. - PubMed
-
-
Crisp JG, Takhar SS, Moran GJ, et al. Inability of polymerase chain reaction, pyrosequencing, and culture of infected and uninfected site skin biopsy specimens to identify the cause of cellulitis. Clin Infect Dis 2015; 61:1679–1687.
■■ The reference is of interest because it describes limitations in advanced diagnostics to help determine the cause of skin and soft tissue infections (SSTIs).
-
-
- Stevens DL, Bisno AL, Chambers HF, et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clin Infect Dis 2014; 59:e10–e52. - PubMed
-
- European Centre for Disease Prevention and Control (ECDC). Annual epi-demiological report 2012: reporting on 2010 surveillance data and 2011 epidemic intelligence data Stockholm: ECDC; 2013.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
