

Team Approach: Osteosarcoma of the Distal Part of the Femur in Adolescents
- PMID: 29278618
- PMCID: PMC5912173
- DOI: 10.2106/JBJS.RVW.17.00030
Team Approach: Osteosarcoma of the Distal Part of the Femur in Adolescents
Abstract
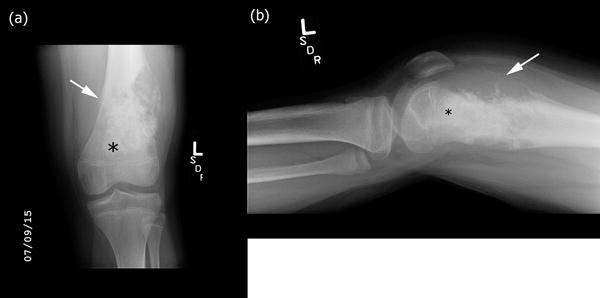
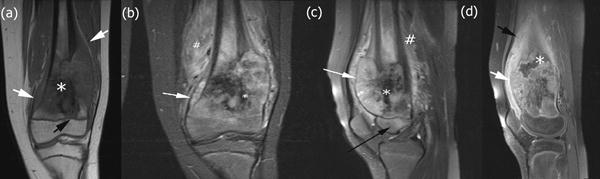
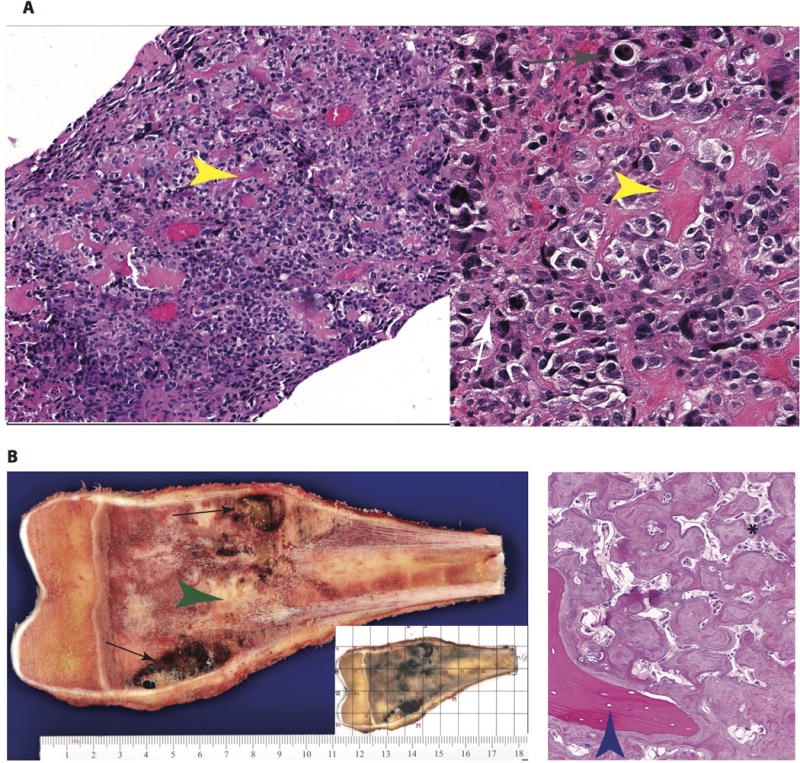
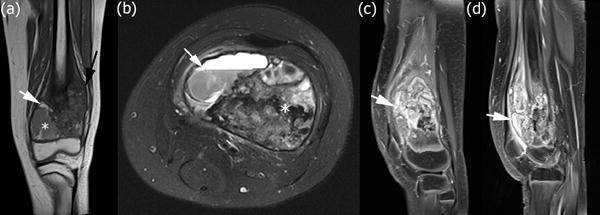
Osteosarcoma, while rare, is the most common primary bone cancer and accounts for up to 10% of all new pediatric cancer diagnoses annually in the United States. Most commonly, osteosarcoma affects the distal femur and occurs as a high-grade intramedullary (conventional) subtype. Patients with osteosarcoma are treated with a multi-disciplinary team approach. Often, an orthopaedic oncologist initiates the workup after making a presumptive diagnosis based on classic clinical and radiographic findings. Advanced imaging and a tissue biopsy are obtained to evaluate the extent of disease and to histologically confirm the diagnosis. Musculoskeletal radiologists and pathologists are key team members who evaluate the imaging and tissue samples to make a definitive diagnosis, establish a prognosis, and help the clinicians develop a treatment plan. Medical/pediatric oncologists are essential team members who provide the appropriate neoadjuvant and adjuvant chemotherapy treatment and assist with long-term surveillance to monitor for local or distant relapse. Orthopaedic oncologists develop and execute a plan for resection of the tumor followed by appropriate reconstruction. The current standard of care for distal femoral osteosarcoma is neoadjuvant chemotherapy followed by limb salvage for the surgically resectable tumor, reconstruction of the bone and soft tissue defect, and adjuvant chemotherapy. The survival for patients with isolated osteosarcoma is approximately 70% and has not substantially improved in over 25 years.–
Figures

Similar articles
-
[ALLOTRANSPLANTATION OF CRYOPRESERVATED VASCULARIZED BONE IN LIMB SALVAGE SURGERY FOR CHILDREN AND ADOLESCENTS WITH OSTEOSARCOMA].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2015 Oct;29(10):1189-93. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2015. PMID: 26749721 Chinese.
-
[Interdisciplinary treatment of osteosarcomas: Part II].Unfallchirurg. 2014 Jul;117(7):582. doi: 10.1007/s00113-014-2569-4. Unfallchirurg. 2014. PMID: 25030956 German. No abstract available.
-
Nonmetastatic osteosarcoma of the extremity with pathologic fracture at presentation: local and systemic control by amputation or limb salvage after preoperative chemotherapy.Acta Orthop Scand. 2003 Aug;74(4):449-54. doi: 10.1080/00016470310017776. Acta Orthop Scand. 2003. PMID: 14521297
-
[Interdisciplinary diagnostic and treatment of bone sarcomas of the extremities and trunk].Handchir Mikrochir Plast Chir. 2015 Apr;47(2):90-9. doi: 10.1055/s-0034-1396853. Epub 2015 Apr 21. Handchir Mikrochir Plast Chir. 2015. PMID: 25897578 Review. German.
-
Joint-preservation surgery for pediatric osteosarcoma of the knee joint.Cancer Metastasis Rev. 2019 Dec;38(4):709-722. doi: 10.1007/s10555-019-09835-z. Cancer Metastasis Rev. 2019. PMID: 31807972 Review.
Cited by
-
Clinicopathological correlations and prognostic insights in osteosarcoma: a retrospective analysis.Rom J Morphol Embryol. 2024 Oct-Dec;65(4):723-736. doi: 10.47162/RJME.65.4.19. Rom J Morphol Embryol. 2024. PMID: 39957034 Free PMC article.
-
Megaprosthesis Total Knee Replacement Following Resection of Extensive Osteoblastic Osteosarcoma in the Distal Femur: A Case Report.Cureus. 2024 Mar 26;16(3):e56971. doi: 10.7759/cureus.56971. eCollection 2024 Mar. Cureus. 2024. PMID: 38665714 Free PMC article.
-
Distal femur osteosarcoma in a seven-year-old: a case report on acute symptom presentation.Ann Med Surg (Lond). 2024 Nov 8;86(12):7449-7453. doi: 10.1097/MS9.0000000000002726. eCollection 2024 Dec. Ann Med Surg (Lond). 2024. PMID: 39649897 Free PMC article.
-
Assessment of the Interval to Diagnosis in Pediatric Bone Sarcoma.Pediatr Emerg Care. 2023 Dec 1;39(12):963-967. doi: 10.1097/PEC.0000000000003031. Epub 2023 Aug 12. Pediatr Emerg Care. 2023. PMID: 37567167 Free PMC article.
-
The presence of a fat layer after neoadjuvant chemotherapy as an indicator of prognosis in osteosarcoma.Front Oncol. 2025 Apr 11;15:1514560. doi: 10.3389/fonc.2025.1514560. eCollection 2025. Front Oncol. 2025. PMID: 40291910 Free PMC article.
References
-
- Wittig JC, Bickels J, Priebat D, et al. Osteosarcoma: a multidisciplinary approach to diagnosis and treatment. Am Fam Physician. 2002;65(6):1123–1132. - PubMed
-
- Dahlin DC, Coventry MB. Osteogenic sarcoma. A study of six hundred cases. J Bone Joint Surg Am. 1967;49(1):101–110. - PubMed
-
- Bielack SS, Kempf-Bielack B, Delling G, et al. Prognostic factors in high-grade osteosarcoma of the extremities or trunk: an analysis of 1,702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols. J Clin Oncol Off J Am Soc Clin Oncol. 2002;20(3):776–790. doi: 10.1200/jco.2002.20.3.776. - DOI - PubMed
-
- Bacci G, Ferrari S, Bertoni F, et al. Long-term outcome for patients with nonmetastatic osteosarcoma of the extremity treated at the istituto ortopedico rizzoli according to the istituto ortopedico rizzoli/osteosarcoma-2 protocol: an updated report. J Clin Oncol Off J Am Soc Clin Oncol. 2000;18(24):4016–4027. doi: 10.1200/jco.2000.18.24.4016. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
