

Association Between Diastolic Blood Pressure During Pediatric In-Hospital Cardiopulmonary Resuscitation and Survival
- PMID: 29279413
- PMCID: PMC5916041
- DOI: 10.1161/CIRCULATIONAHA.117.032270
Association Between Diastolic Blood Pressure During Pediatric In-Hospital Cardiopulmonary Resuscitation and Survival
Abstract
Background: On the basis of laboratory cardiopulmonary resuscitation (CPR) investigations and limited adult data demonstrating that survival depends on attaining adequate arterial diastolic blood pressure (DBP) during CPR, the American Heart Association recommends using blood pressure to guide pediatric CPR. However, evidence-based blood pressure targets during pediatric CPR remain an important knowledge gap for CPR guidelines.
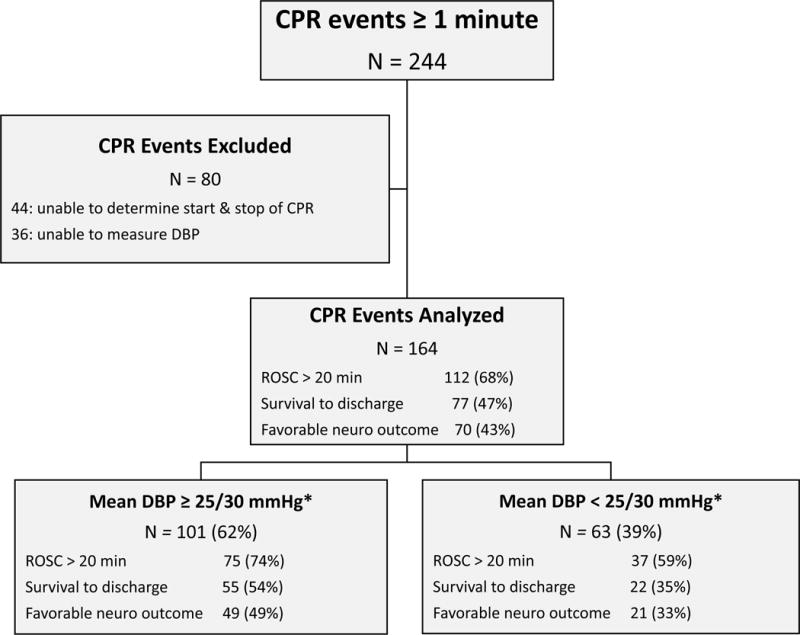
Methods: All children ≥37 weeks' gestation and <19 years old in Collaborative Pediatric Critical Care Research Network intensive care units with chest compressions for ≥1 minute and invasive arterial blood pressure monitoring before and during CPR between July 1, 2013, and June 31, 2016, were included. Mean DBP during CPR and Utstein-style standardized cardiac arrest data were collected. The hypothesis was that DBP ≥25 mm Hg during CPR in infants and ≥30 mm Hg in children ≥1 year old would be associated with survival. Primary outcome was survival to hospital discharge. Secondary outcome was survival to hospital discharge with favorable neurological outcome, defined as Pediatric Cerebral Performance Categories 1 to 3 or no worse than prearrest baseline. Multivariable Poisson regression models with robust error estimates were used to estimate the relative risk of outcomes.
Results: Blinded investigators analyzed blood pressure waveforms during CPR from 164 children, including 60% <1 year old, 60% with congenital heart disease, and 54% after cardiac surgery. The immediate cause of arrest was hypotension in 67%, respiratory decompensation in 44%, and arrhythmia in 19%. Median duration of CPR was 8 minutes (quartiles, 3 and 27 minutes). Ninety percent survived the event, 68% with return of spontaneous circulation and 22% by extracorporeal life support. Forty-seven percent survived to hospital discharge, and 43% survived to discharge with favorable neurological outcome. Maintaining mean DBP ≥25 mm Hg in infants and ≥30 mm Hg in children ≥1 year old occurred in 101 of 164 children (62%) and was associated with survival (adjusted relative risk, 1.7; 95% confidence interval, 1.2-2.6; P=0.007) and survival with favorable neurological outcome (adjusted relative risk, 1.6; 95% confidence interval, 1.1-2.5; P=0.02).
Conclusions: These data demonstrate that mean DBP ≥25 mm Hg during CPR in infants and ≥30 mm Hg in children ≥1 year old was associated with greater likelihood of survival to hospital discharge and survival with favorable neurological outcome.
Keywords: cardiopulmonary resuscitation; heart arrest; pediatrics; survival; treatment outcomes.
© 2017 American Heart Association, Inc.
Figures



Comment in
-
Letter by Guo et al Regarding Article, "Association Between Diastolic Blood Pressure During Pediatric In-Hospital Cardiopulmonary Resuscitation and Survival".Circulation. 2018 Nov 27;138(22):2586-2587. doi: 10.1161/CIRCULATIONAHA.118.035691. Circulation. 2018. PMID: 30571352 No abstract available.
-
Response by Berg et al to Letter Regarding Article, "Association Between Diastolic Blood Pressure During Pediatric In-Hospital Cardiopulmonary Resuscitation and Survival".Circulation. 2018 Nov 27;138(22):2588-2589. doi: 10.1161/CIRCULATIONAHA.118.037291. Circulation. 2018. PMID: 30571353 Free PMC article. No abstract available.
References
-
- Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, Deo R, de Ferranti SD, Floyd J, Fornage M, Gillespie C, Isasi CR, Jiménez MC, Jordan LC, Judd SE, Lackland D, Lichtman JH, Lisabeth L, Liu S, Longenecker CT, Mackey RH, Matsushita K, Mozaffarian D, Mussolino ME, Nasir K, Neumar RW, Palaniappan L, Pandey DK, Thiagarajan RR, Reeves MJ, Ritchey M, Rodriguez CJ, Roth GA, Rosamond WD, Sasson C, Towfighi A, Tsao CW, Turner MB, Virani SS, Voeks JH, Willey JZ, Wilkins JT, Wu JH, Alger HM, Wong SS, Muntner P. Heart Disease and Stroke Statistics—2017 Update: A Report From the American Heart Association. Circulation. 2017;135:e146–e603. - PMC - PubMed
-
- Meaney PA, Bobrow BJ, Mancini ME, Christenson J, de Caen AR, Bhanji F, Abella BS, Kleinman ME, Edelson DP, Berg RA, Aufderheide TP, Menon V, Leary M. Cardiopulmonary resuscitation quality: improving cardiac resuscitation outcomes both inside and outside the hospital: a consensus statement from the American Heart Association. Circulation. 2013;128:417–435. - PubMed
-
- Link MS, Berkow LC, Kudenchuk PJ, Halperin HR, Hess EP, Moitra VK, Neumar RW, O’Neil BJ, Paxton JH, Silvers SM, White RD, Yannopoulos D, Donnino MW. Part 7: Adult Advanced Cardiovascular Life Support: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2015;132:S444–464. - PubMed
-
- de Caen AR, Berg MD, Chameides L, Gooden CK, Hickey RW, Scott HF, Sutton RM, Tijssen JA, Topjian A, van der Jagt ÉW, Schexnayder SM, Samson RA. Part 12: Pediatric Advanced Life Support. 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2015;136:S176–S195. - PubMed
Publication types
MeSH terms
Grants and funding
- U10 HD063108/HD/NICHD NIH HHS/United States
- U10 HD050012/HD/NICHD NIH HHS/United States
- UG1 HD050012/HD/NICHD NIH HHS/United States
- UG1 HD049983/HD/NICHD NIH HHS/United States
- UG1 HD050096/HD/NICHD NIH HHS/United States
- U10 HD049981/HD/NICHD NIH HHS/United States
- U10 HD050096/HD/NICHD NIH HHS/United States
- U10 HD049983/HD/NICHD NIH HHS/United States
- U10 HD063106/HD/NICHD NIH HHS/United States
- UG1 HD063108/HD/NICHD NIH HHS/United States
- RL1 HD107773/HD/NICHD NIH HHS/United States
- UG1 HD063106/HD/NICHD NIH HHS/United States
- UG1 HD083171/HD/NICHD NIH HHS/United States
- U10 HD063114/HD/NICHD NIH HHS/United States
- U01 HD049934/HD/NICHD NIH HHS/United States
- UG1 HD049981/HD/NICHD NIH HHS/United States
- UG1 HD083170/HD/NICHD NIH HHS/United States
- UG1 HD083166/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
