

An Interventional Quality Improvement Study to Assess the Compliance to Cardiopulmonary Resuscitation Documentation in an Indian Teaching Hospital
- PMID: 29279637
- PMCID: PMC5699004
- DOI: 10.4103/ijccm.IJCCM_249_17
An Interventional Quality Improvement Study to Assess the Compliance to Cardiopulmonary Resuscitation Documentation in an Indian Teaching Hospital
Abstract
Background: Cardiopulmonary resuscitation (CPR) should be performed as per the international guidelines; however, compliance to these guidelines is difficult to assess. This study was conducted to determine the compliance to American Heart Association (2010) guideline on CPR documentation by among resident physicians before and after resident training (two arms).
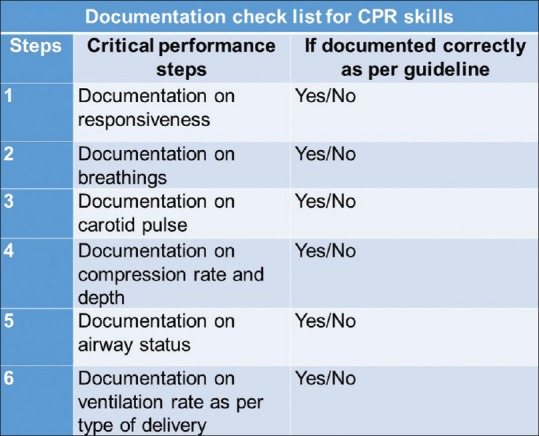
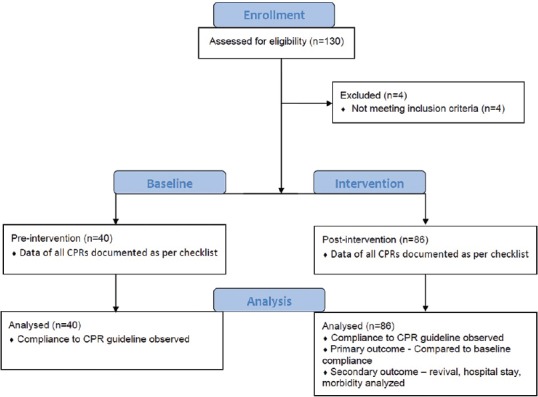
Methods: This pre-postinterventional quality improvement study was conducted in a referral center, North India. Data of hospitalized in-hospital CPR patients were collected in the form of quality indicators (checklists) as defined by the guideline and compared between two arms of before-after resident training. Residents were given appropriate training in CPR technique as per the guideline. The compliance of CPR documentation was assessed pre- and post-intervention.
Results: The baseline arm compliance of various components of CPR documentation was low. The postintervention arm compliances of all components significantly increased (baseline, 2.5% to postintervention, 15.11%, P = 0.03). Individual components assessed were documentation of assessment of responsiveness (65% to 77.9%, P = 0.19), assessment of breathing (37.5% to 58.1%, P = 0.03), assessment of carotid pulse (62.5% to 79%, P = 0.05), rate of chest compressions (20% to 39.5%, P = 0.04), airway management (62.5% to 82.5%, P = 0.02), and compressions to breaths ratio (12.5% to 31.4%, P = 0.02). Documentation of chest compression rate compared to nondocumentation (12 of 42 vs. 11 of 84, P = 0.04) was independently associated with a higher rate of return of spontaneous circulation. The study however did not show any survival benefits.
Conclusions: This study establishes that the compliance to CPR documentation is poor as assessed by CPR documentation content and quality, which improves after physician training, but not up to the mark level (100%) that may be due to busy Indian hospital settings and human behavioral factors. Due to ethical constraints of live CPR assessment, this document checklist approach may be considered as an internal quality assessment method for CPR compliance. Furthermore, correct instruction in CPR technique along with proper documentation of the procedure is required, followed up with periodic re-education during the residency period and beyond.
Keywords: Adults; cardiopulmonary resuscitation documentation; in-hospital cardiac arrest; quality appraisal.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Sasson C, Rogers MA, Dahl J, Kellermann AL. Predictors of survival from out-of-hospital cardiac arrest: A systematic review and meta-analysis. Circ Cardiovasc Qual Outcomes. 2010;3:63–81. - PubMed
-
- Eisenberg MS, Mengert TJ. Cardiac resuscitation. N Engl J Med. 2001;344:1304–13. - PubMed
-
- Rea TD, Crouthamel M, Eisenberg MS, Becker LJ, Lima AR. Temporal patterns in long-term survival after resuscitation from out-of-hospital cardiac arrest. Circulation. 2003;108:1196–201. - PubMed
-
- Van Hoeyweghen RJ, Bossaert LL, Mullie A, Calle P, Martens P, Buylaert WA, et al. Quality and efficiency of bystander CPR. Belgian Cerebral Resuscitation Study Group. Resuscitation. 1993;26:47–52. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources