

Neuroimaging of Dilated Perivascular Spaces: From Benign and Pathologic Causes to Mimics
- PMID: 29280227
- PMCID: PMC6398334
- DOI: 10.1111/jon.12493
Neuroimaging of Dilated Perivascular Spaces: From Benign and Pathologic Causes to Mimics
Abstract
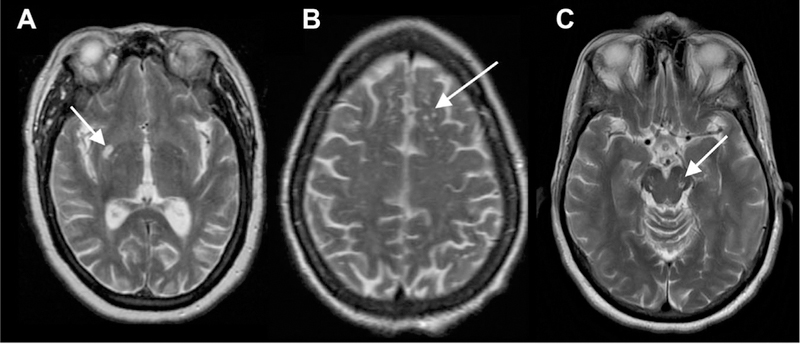
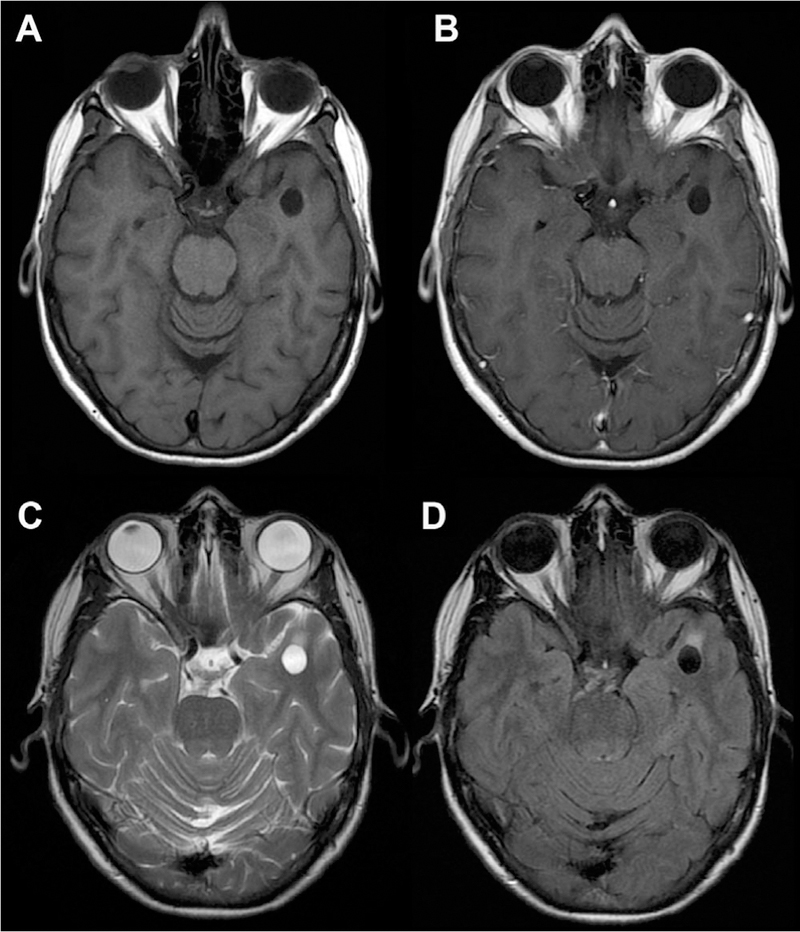
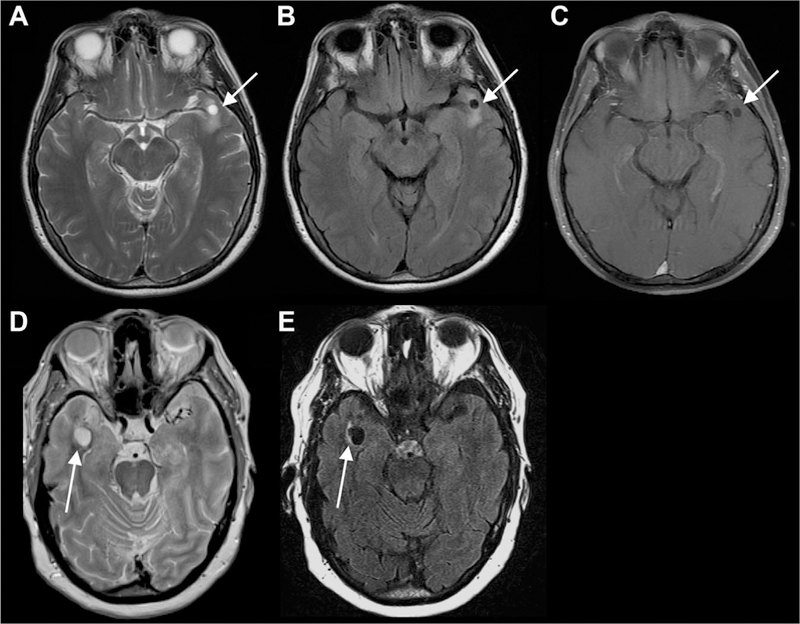
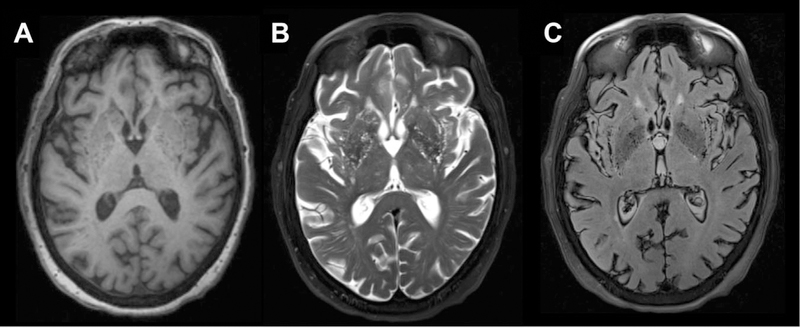
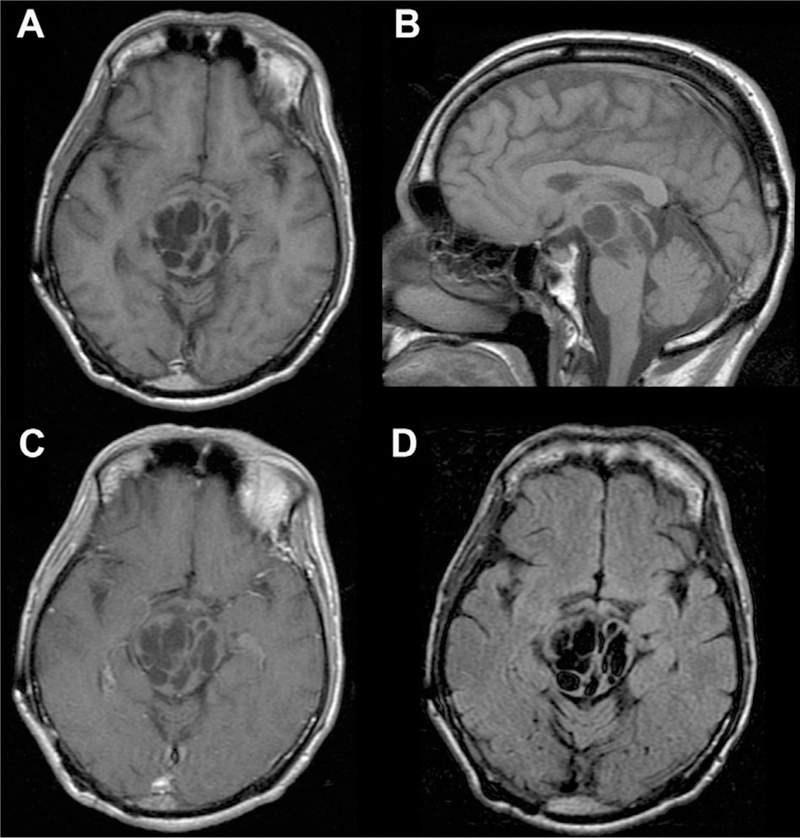
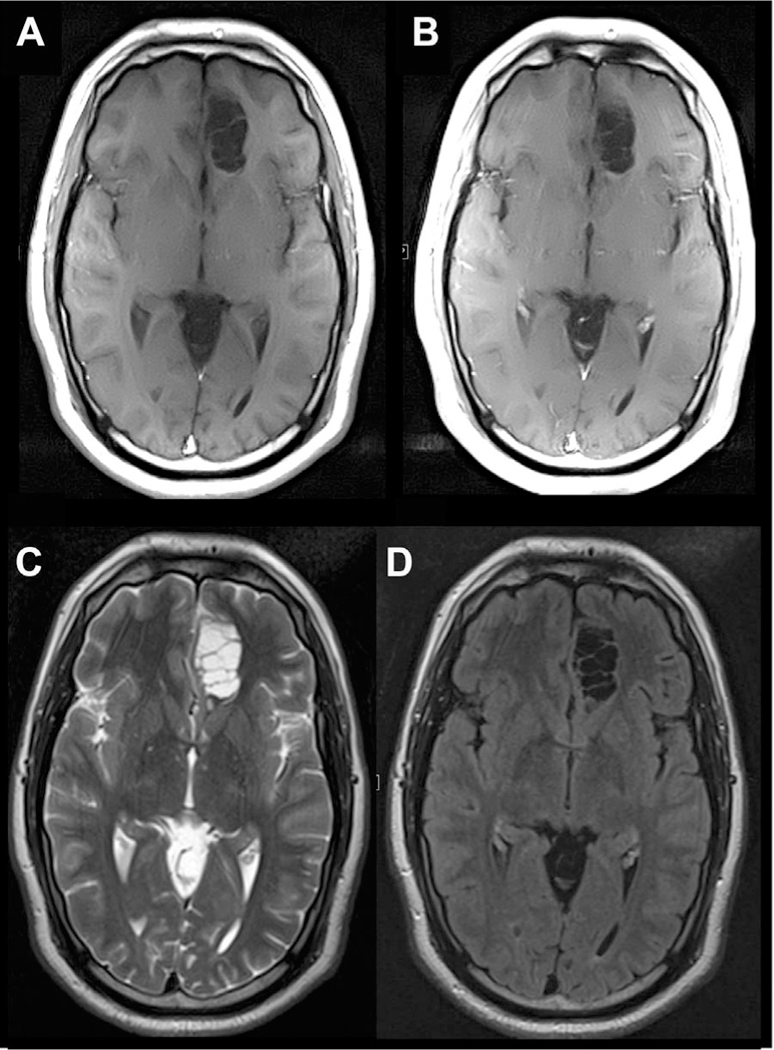
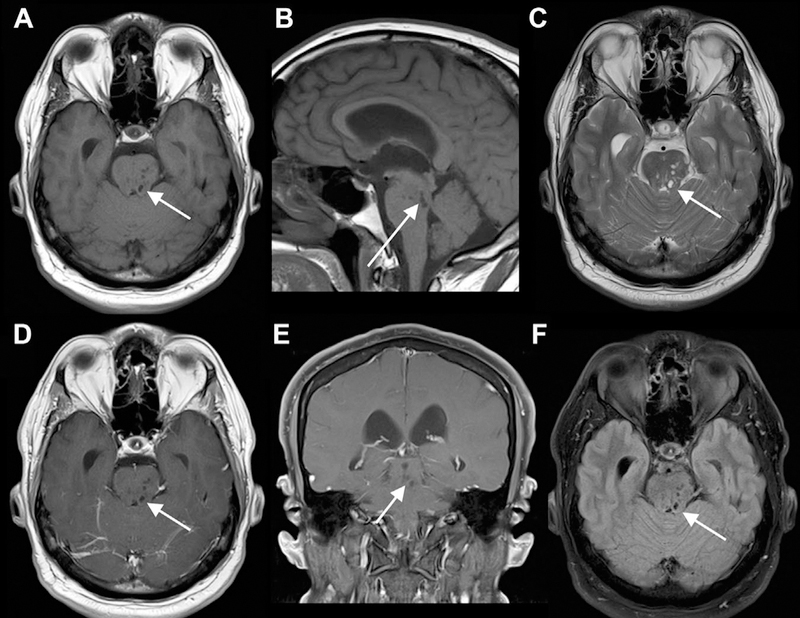
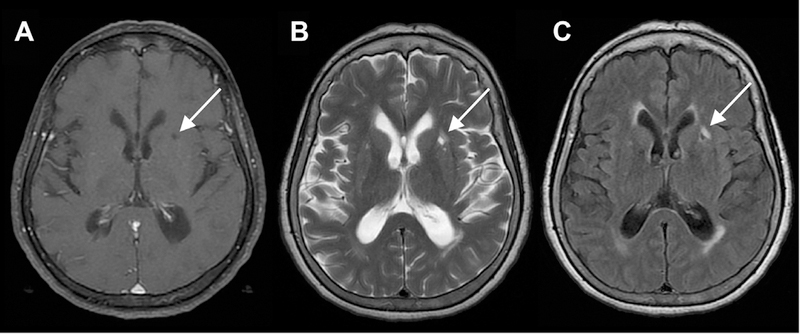
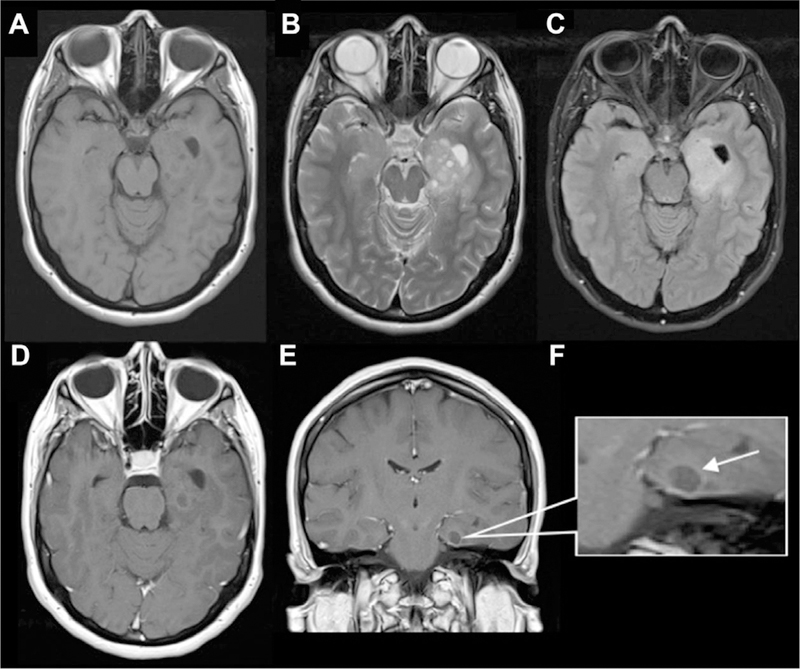
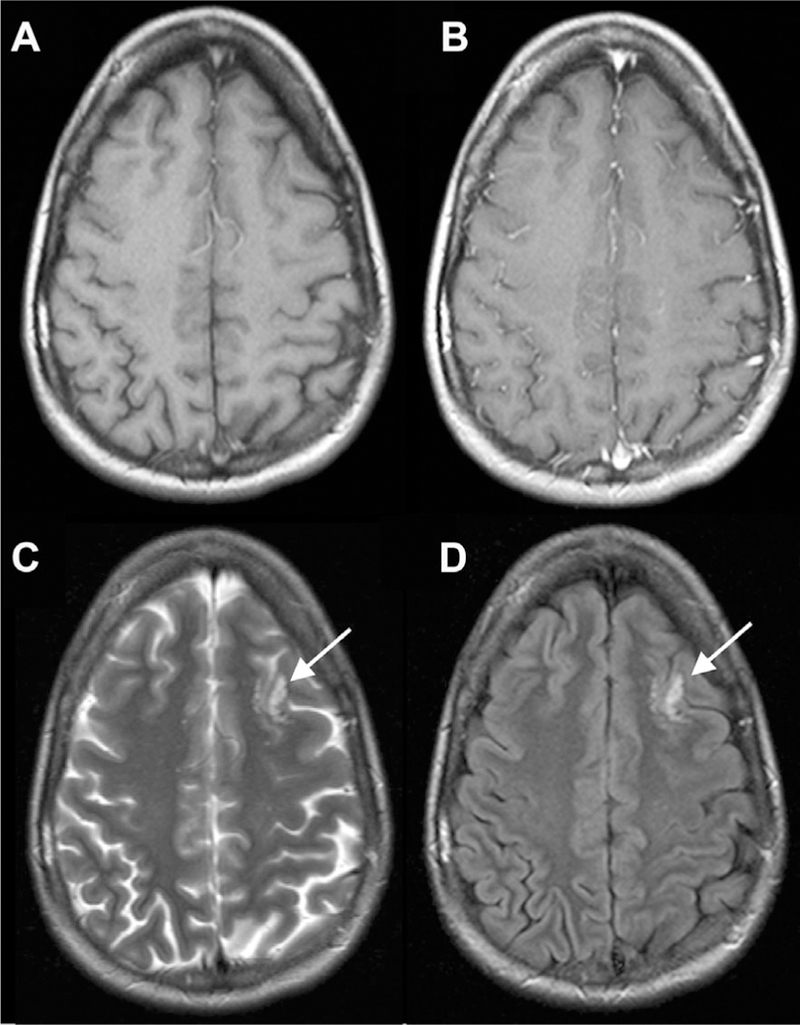
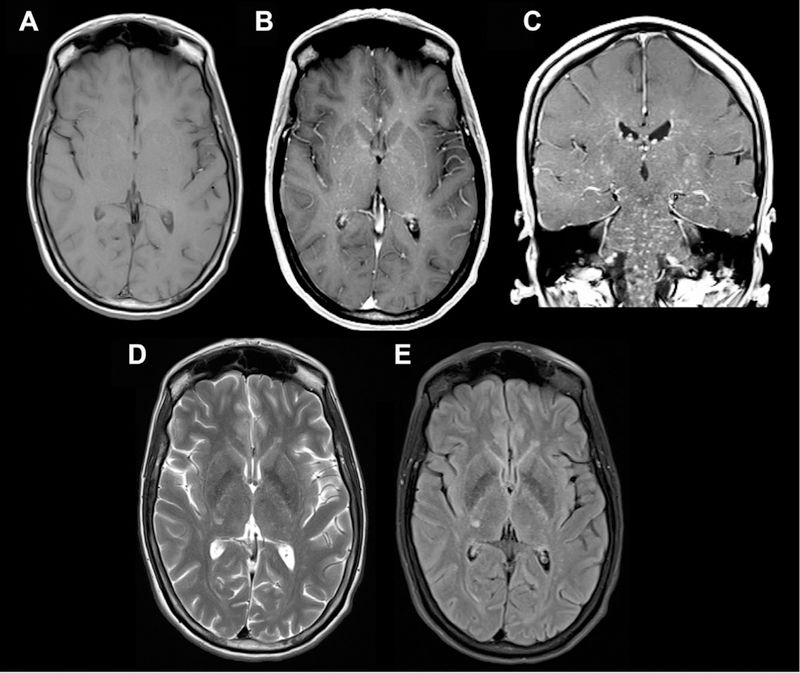
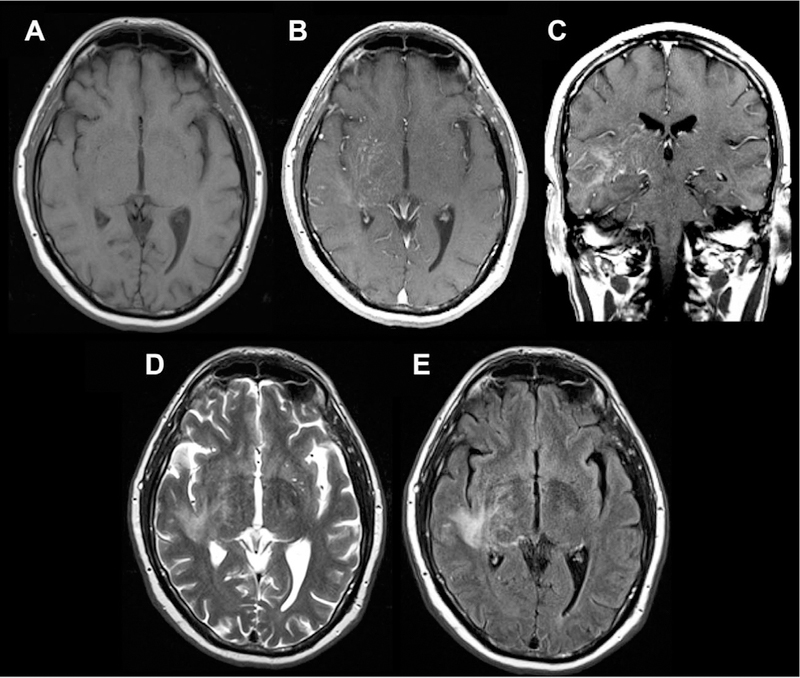
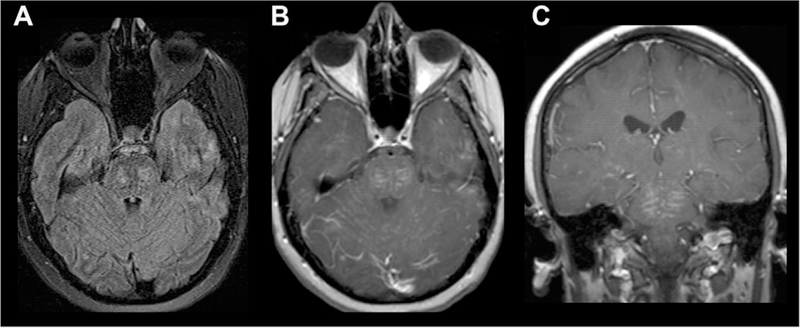
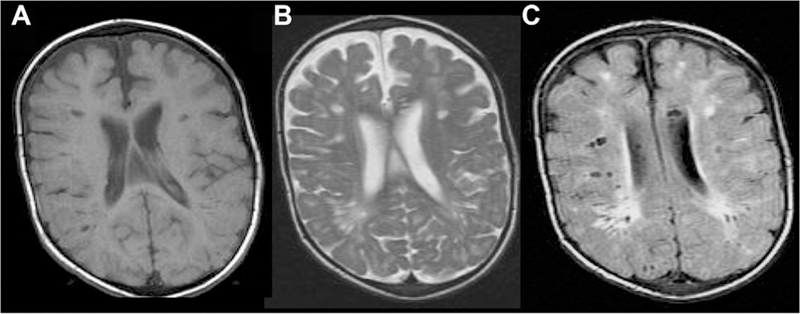
Perivascular spaces (PVSs), also known as Virchow-Robin spaces, are pial-lined, fluid-filled structures found in characteristic locations throughout the brain. They can become abnormally enlarged or dilated and in rare cases can cause hydrocephalus. Dilated PVSs can pose a diagnostic dilemma for radiologists because of their varied appearance, sometimes mimicking more serious entities such as cystic neoplasms, including dysembryoplastic neuroepithelial tumor and multinodular and vacuolating neuronal tumor, or cystic infections including toxoplasmosis and neurocysticercosis. In addition, various pathologic processes, including cryptococcosis and chronic lymphocytic inflammation with pontine perivascular enhancement responsive to steroids, can spread into the brain via PVSs, resulting in characteristic magnetic resonance imaging appearances. This review aims to describe the key imaging characteristics of normal and dilated PVSs, as well as cystic mimics and pathologic processes that directly involve PVSs.
Keywords: Neuroradiology; Virchow-Robin spaces; perivascular spaces.
Copyright © 2017 by the American Society of Neuroimaging.
Conflict of interest statement
Figures
References
-
- Virchow R Ueber die erweiterung kleinerer gefaesse. Arch Pathol Anat Physiol Klin Med 1851;3:427–62.
-
- Robin C Recherches sur quelques particularites de la structure des capillaires de l’encephale. J Physiol Homme Animaux 1859;2:537–48.
-
- Schley D, Carare-Nnadi R, Please CP, et al. Mechanisms to explain the reverse perivascular transport of solutes out of the brain. J Theor Biol 2006;238:962–74. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
