

Health care costs associated with hospital acquired complications in patients with chronic kidney disease
- PMID: 29282006
- PMCID: PMC5745961
- DOI: 10.1186/s12882-017-0784-2
Health care costs associated with hospital acquired complications in patients with chronic kidney disease
Abstract
Background: Patients with CKD are at increased risk of potentially preventable hospital acquired complications (HACs). Understanding the economic consequences of preventable HACs, may define the scope and investment of initiatives aimed at prevention.
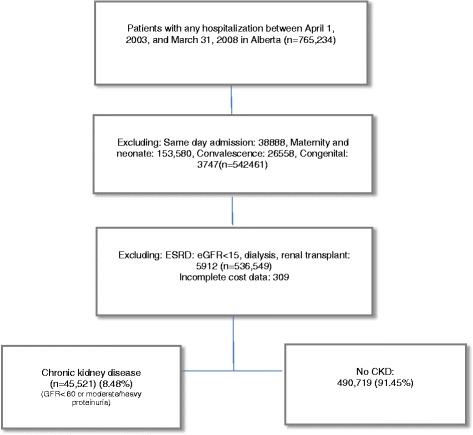
Methods: Adult patients hospitalized from April, 2003 to March, 2008 in Alberta, Canada comprised the study cohort. Healthcare costs were determined and categorized into 'index hospitalization' including hospital cost and in-hospital physician claims, and 'post discharge' including ambulatory care cost, physician claims, and readmission costs from discharge to 90 days. Multivariable regression was used to estimate the incremental healthcare costs associated with potentially preventable HACs.
Results: In fully adjusted models, the median incremental index hospitalization cost was CAN-$6169 (95% CI; 6003-6336) in CKD patients with ≥1 potentially preventable HACs, compared with those without. Post-discharge incremental costs were 1471(95% CI; 844-2099) in those patients with CKD who developed potentially preventable HACs within 90 days after discharge compared with patients without potentially preventable HACs. Additionally, the incremental costs associated with ≥1 potentially preventable HACs within 90 days from admission in patients with CKD were $7522 (95% CI; 7219-7824). A graded relation of the incremental costs was noted with the increasing number of complications. In patients without CKD but with ≥1 preventable HACs incremental costs within 90 days from hospital admission was $6688 (95% CI: 6612-6723).
Conclusions: Potentially preventable HACs are associated with substantial increases in healthcare costs in people with CKD. Investment in implementing targeted strategies to reduce HACs may have a significant benefit for patient and health system outcomes.
Keywords: Chronic kidney disease; Healthcare costs; Hospital acquired complication; Readmission.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by Ethics board of university of Alberta on October 17, 2016 with the ID number of MS3_00036226.
Member, Health Research Ethics Board (HERB) - Health Panel, University of Alberta. Our HERB did not require patient written or verbal consent as this was use of already collect data.
Consent for publication
“Not applicable”. Manuscript does not contain data from any individual person.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Jackson T, Fong A, Liu M, Murray K, Walz L, Houston C, et al. Incremental costs of hospital-acquired complications in Alberta, Canada. BMC Health Serv Res. 2011;11(Suppl 1):A15. doi: 10.1186/1472-6963-11-S1-A15. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
