

Spectrum (characteristics) of patients with chronic kidney disease (CKD) with increasing age in a major metropolitan renal service
- PMID: 29282014
- PMCID: PMC5745771
- DOI: 10.1186/s12882-017-0781-5
Spectrum (characteristics) of patients with chronic kidney disease (CKD) with increasing age in a major metropolitan renal service
Abstract
Background: Aim of our study is to describe, in people with CKD, the demographic and clinical characteristics and outcomes with increasing age. The prevalence of CKD in Western populations, where longevity is the norm, is about 10-15%, but how age influence different characteristics of patients with CKD is largely not known.
Methods: One thousand two hundred sixty-five patients enrolled in the CKD.QLD registry at the Royal Brisbane and Women's Hospital were grouped according to age at consent i.e. <35, 35-44, 45-54, 55-64, 65-74, 75-84, 85+ years age groups, and were followed till start of renal replacement therapy (RRT), death, discharge or the censor date of September 2015.
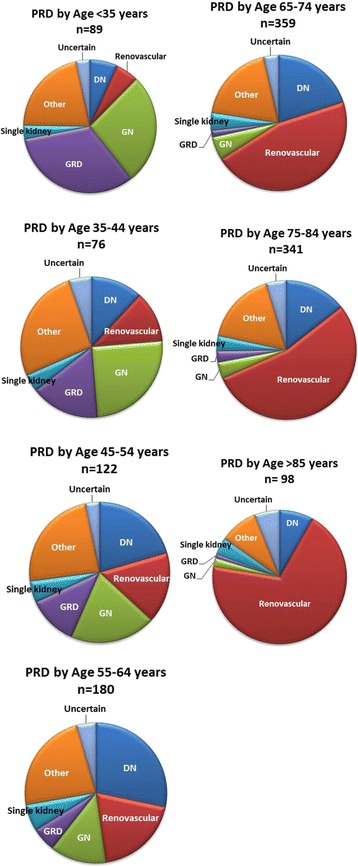
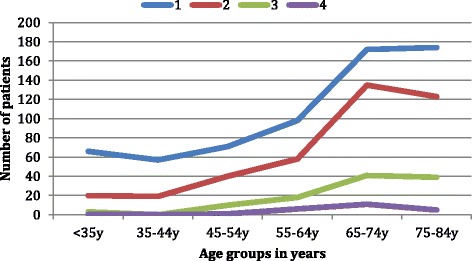
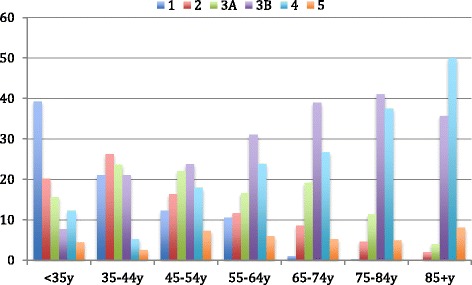
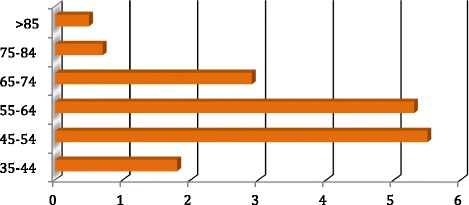
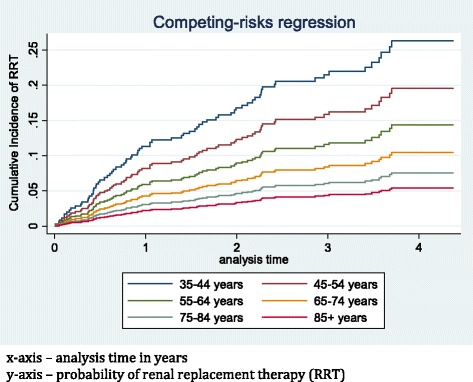
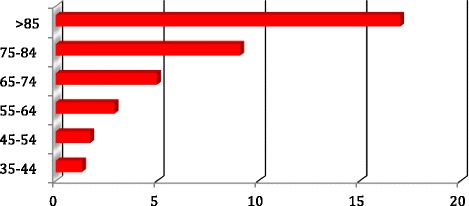
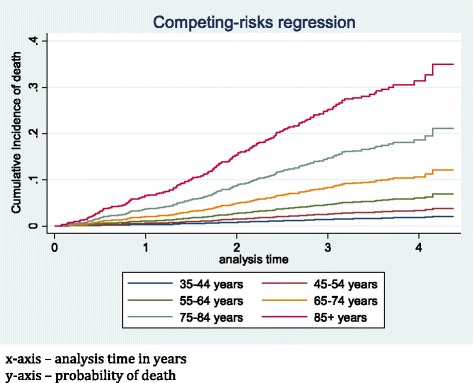
Results: Age ranged from 17.6 to 98.5 years with medians of 70.1 and 69.9 years for males and females respectively: 7% were <35 years of age, with the majority (63%) >65 years old. The leading renal diagnoses changed from genetic real disease (GRD) and glomerulonephritis (GN) in the younger patients to renovascular disease (RVD) and hypertension (HTN) in older patients. With increasing age, there were often multiple renal disease diagnoses, more advanced stages of CKD, greater number of comorbidities, more frequent and more costly hospitalizations, and higher death rates. The rates of initiation of renal replacement therapy (RRT) rose from 4.5 per 100 person years in those age < 35 years to a maximum of 5.5 per 100 person years in 45-54 years age group and were lowest, at 0.5 per 100 person years in those >85 years. Mortality rates increased by age group from 1.3 to 17.0 per 100 person years in 35-44 year and 85+ year age groups respectively. Rates of hospitalization, length of stay and cost progressively increased from the youngest to eldest groups. Patients with diabetic nephropathy had highest incidence rate of RRT and death. The proportion of patients who lost more than 5mls/min/1.73m2 of eGFR during at least 12 months follow up increased from 13.3% in the youngest age group to 29.2% in the eldest.
Conclusion: This is the first comprehensive view, with no exclusions, of CKD patients seen in a public renal specialty referral practice, in Australia. The age distribution of patients encompasses the whole of adult life, with a broader range and higher median value than patients receiving RRT. Health status ranged from a single system (renal) disease in young adults through, with advancing age, renal impairment as a component of, or accompanying multisystem diseases, to demands and complexities of support of frail or elderly people approaching end of life. This great spectrum demands a broad understanding and capacity of renal health care providers, and dictates a need for a wider scope of health services provision incorporating multiple models of care.
Keywords: Age distribution; CKD.QLD registry; Chronic kidney disease; Clinical characteristics; Death; Heterogeneity; Hospitalization; Outcomes; Progression; Renal replacement therapy.
Conflict of interest statement
Ethics approval and consent to participate
“Chronic Kidney Disease in Queensland (CKD.QLD) Registry Study” has Royal Brisbane and Women’s Hospital Human Research Ethics Committee approval - HREC Reference Number (MNHHS): HREC/15/QRBW/294 as of June 2015 (Previous HREC Reference Number (OHMR): HREC/10/QHC/41 from Nov 2010 to June 2015 University of Queensland Medical Research Ethics Number: 2011000029). All participants were adults and gave written informed consent to participate in the study.
Consent for publication
“Not Applicable”
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Chronic kidney disease, Queensland: Profile of patients with chronic kidney disease from regional Queensland, Australia: A registry report.Nephrology (Carlton). 2019 Dec;24(12):1257-1264. doi: 10.1111/nep.13567. Epub 2019 May 2. Nephrology (Carlton). 2019. PMID: 30663166
-
Low renal replacement therapy incidence among slowly progressing elderly chronic kidney disease patients referred to nephrology care: an observational study.BMC Nephrol. 2017 Feb 10;18(1):59. doi: 10.1186/s12882-017-0473-1. BMC Nephrol. 2017. PMID: 28187786 Free PMC article.
-
Translating chronic kidney disease epidemiology into patient care--the individual/public health risk paradox.Nephrol Dial Transplant. 2012 Oct;27 Suppl 3:iii65-72. doi: 10.1093/ndt/gfr746. Epub 2012 Apr 24. Nephrol Dial Transplant. 2012. PMID: 22532617
-
Hyperphosphataemia in Chronic Kidney Disease: Management of Hyperphosphataemia in Patients with Stage 4 or 5 Chronic Kidney Disease.Manchester: National Institute for Health and Clinical Excellence (UK); 2013 Mar. Manchester: National Institute for Health and Clinical Excellence (UK); 2013 Mar. PMID: 25340244 Free Books & Documents. Review.
-
Sex and gender disparities in the epidemiology and outcomes of chronic kidney disease.Nat Rev Nephrol. 2018 Mar;14(3):151-164. doi: 10.1038/nrneph.2017.181. Epub 2018 Jan 22. Nat Rev Nephrol. 2018. PMID: 29355169 Review.
Cited by
-
Chronic kidney disease in public renal practices in Queensland, Australia, 2011-2018.Nephrology (Carlton). 2022 Dec;27(12):934-944. doi: 10.1111/nep.14111. Epub 2022 Oct 9. Nephrology (Carlton). 2022. PMID: 36161428 Free PMC article.
-
Pathological spectrum of glomerular disease in patients with renal insufficiency: a single-center study in Northeastern China.Ren Fail. 2019 Nov;41(1):473-480. doi: 10.1080/0886022X.2019.1620774. Ren Fail. 2019. PMID: 31198075 Free PMC article.
-
[The research and application advances of medical imaging techniques in early renal function assessment of chronic kidney disease].Sheng Wu Yi Xue Gong Cheng Xue Za Zhi. 2019 Jun 25;36(3):511-514. doi: 10.7507/1001-5515.201901028. Sheng Wu Yi Xue Gong Cheng Xue Za Zhi. 2019. PMID: 31232557 Free PMC article. Review. Chinese.
-
The Effects of Gum Acacia on the Composition of the Gut Microbiome and Plasma Levels of Short-Chain Fatty Acids in a Rat Model of Chronic Kidney Disease.Front Pharmacol. 2020 Dec 22;11:569402. doi: 10.3389/fphar.2020.569402. eCollection 2020. Front Pharmacol. 2020. PMID: 33628167 Free PMC article.
-
Risk Prediction for Early Chronic Kidney Disease: Results from an Adult Health Examination Program of 19,270 Individuals.Int J Environ Res Public Health. 2020 Jul 10;17(14):4973. doi: 10.3390/ijerph17144973. Int J Environ Res Public Health. 2020. PMID: 32664271 Free PMC article.
References
-
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the global burden of disease study 2010. Lancet (London, England) 2012;380(9859):2095–2128. doi: 10.1016/S0140-6736(12)61728-0. - DOI - PMC - PubMed
-
- Cass ACS, Gallagher M, Howard K, Jones A, McDonald S, et al. The economic impact of end-stage kidney disease in Australia: Projections to 2020. Melbourne: Kidney Health Australia; 2010.
-
- Cardiovascular disease, diabetes and chronic kidney disease: Australian facts: prevalence and incidence . Cardiovascular, diabetes and chronic kidney disease series no. 2. Cat. no. CDK 2. Canberra: AIHW; 2014.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
