

Enhanced recovery after surgery program in Gynaecologic Oncological surgery in a minimally invasive techniques expert center
- PMID: 29282059
- PMCID: PMC5745717
- DOI: 10.1186/s12893-017-0332-9
Enhanced recovery after surgery program in Gynaecologic Oncological surgery in a minimally invasive techniques expert center
Abstract
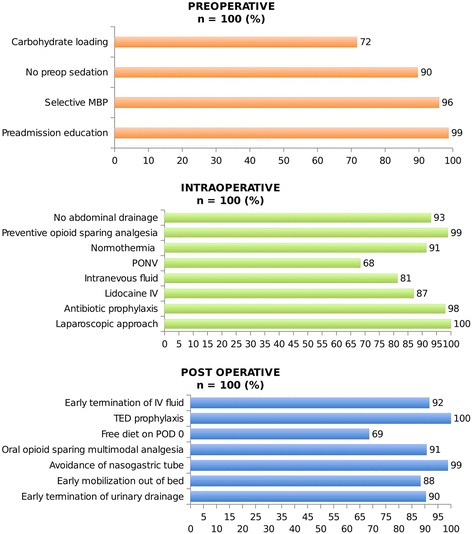
Background: Enhanced Recovery After Surgery Programs (ERP) includes multimodal approaches of perioperative patient's clinical pathways designed to achieve early recovery after surgery and a decreased length of hospital stay (LOS).
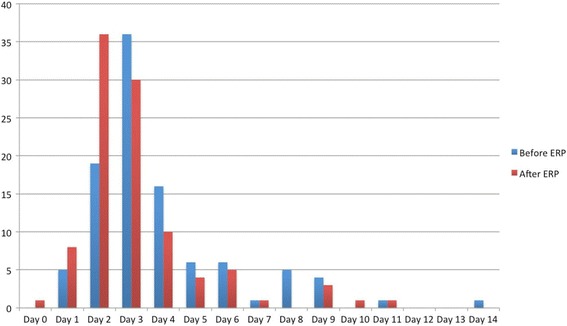
Methods: This observational study evaluated the implementation of ERP in gynaecologic oncological surgery in a minimally invasive techniques (MIT) expert center with more than 85% of procedures done with MIT. We compared a prospective cohort of 100 patients involved in ERP between December 2015 and June 2016 to a 100 patients control group, without ERP, previously managed in the same center between April 2015 and November 2015. All the included patients were referred for hysterectomy and/or pelvic or para-aortic lymphadenectomy for gynaecological cancer. The primary objective was to achieve a significant decrease of median LOS in the ERP group. Secondary objectives were decreases in proportion of patients achieving target LOS (2 days), morbidity and readmissions.
Results: Except a disparity in oncological indications with a higher proportion of endometrial cancer in the group with ERP vs. the group without ERP (42% vs. 22%; p = 0.003), there were no differences in patient's characteristics and surgical procedures. ERP were associated with decreases of median LOS (2.5 [0 to 11] days vs. 3 [1 to 14] days; p = 0.002) and proportion of discharged patient at target LOS (45% vs. 24%; p = 0.002). Morbidities occurred in 25% and 26% in the groups with and without ERP and readmission rates were respectively of 6% and 8%, without any significant difference.
Conclusion: ERP in gynaecologic oncological surgery is associated with a decrease of LOS without increases of morbidity or readmission rates, even in a center with a high proportion of MIT. Although it is already widely accepted that MIT improves early recovery, our study shows that the addition of ERP's clinical pathways improve surgical outcomes and patient care management.
Keywords: Enhanced recovery after surgery; Fast-track programs; Gynaecological oncology surgery; Medical care enhancement; Minimally invasive techniques.
Conflict of interest statement
Ethics approval and consent to participate
This work was approved by our institutional review board (IPC - Comité d’Orientation Stratégique).
All procedures performed in this study involving human participants were done in accordance with the French ethical standards and with the 2008 Helsinki declaration.
All included patients provided written informed consent before surgery.
Consent for publication
Not applicable.
Competing interests
The Authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
