

Current status of theranostics in prostate cancer
- PMID: 29282518
- PMCID: PMC5787224
- DOI: 10.1007/s00259-017-3882-2
Current status of theranostics in prostate cancer
Abstract
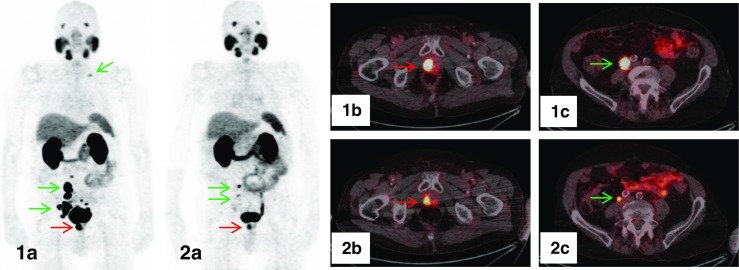
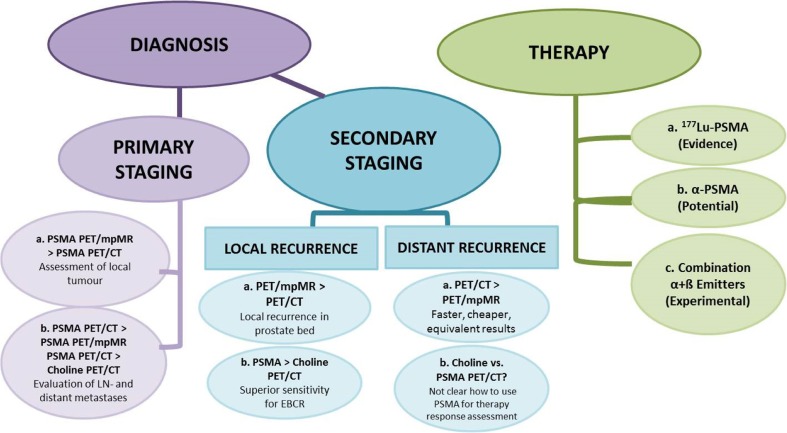
The aim of this review is to report on the current status of prostate-specific membrane antigen (PSMA)-directed theranostics in prostate cancer (PC) patients. The value of 68Ga-PSMA-directed PET imaging as a diagnostic procedure for primary and recurrent PC as well as the role of evolving PSMA radioligand therapy (PRLT) in castration-resistant (CR)PC is assessed. The most eminent data from mostly retrospective studies currently available on theranostics of prostate cancer are discussed. The current knowledge on 68Ga-PSMA PET/CT implicates that primary staging with PET/CT is meaningful in patients with high-risk PC and that the combination with pelvic multi parametric (mp)MR (or PET/mpMR) reaches the highest impact on patient management. There may be a place for 68Ga-PSMA PET/CT in intermediate-risk PC patients as well, however, only a few data are available at the moment. In secondary staging for local recurrence, 68Ga-PSMA PET/mpMR is superior to PET/CT, whereas for distant recurrence, PET/CT has equivalent results and is faster and cheaper compared to PET/mpMR. 68Ga-PSMA PET/CT is superior to 18F / 11Choline PET/CT in primary staging as well as in secondary staging. In patients with biochemical relapse, PET/CT positivity is directly associated with prostate-specific antigen (PSA) increase and amounts to roughly 50% when PSA is raised to ≤0.5 ng/ml and to ≥90% above 1 ng/ml. Significant clinical results have so far been achieved with the subsequent use of radiolabeled PSMA ligands in the treatment of CRPC. Accumulated activities of 30 to 50 GBq of 177Lu-PSMA ligands seem to be clinically safe with biochemical response and PERCIST/RECIST response in around 75% of patients along with xerostomia in 5-10% of patients as the only notable side effect. On the basis of the current literature, we conclude that PSMA-directed theranostics do have a major clinical impact in diagnosis and therapy of PC patients. We recommend that 68Ga-PSMA PET/CT should be performed in primary staging together with pelvic mpMR in high-risk patients and in all patients for secondary staging, and that PSMA-directed therapy is a potent strategy in CRPC patients when other treatment options have failed. The combination of PSMA-directed therapy with existing therapy modalities (such as 223Ra-chloride or androgen deprivation therapy) has to be explored, and prospective clinical multicenter trials with theranostics are warranted.
Keywords: 68Ga-PSMA; PET-guided personalized therapy; PET/CT; PET/MR; Prostanostics; Prostate cancer; Theranostics.
Conflict of interest statement
Disclosure
The authors declare no conflict of interest relevant to this article.
Conflict of interest
The authors declare that they have no financial or non-financial competing interests.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
This article does not contain any studies with animals performed by any of the authors.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Figures
References
-
- ProstaScint. https://www.drugs.com/pro/prostascint.html. Accessed 13 June 2017.
-
- Bander NH, Trabulsi EJ, Kostakoglu L, Yao D, Vallabhajosula S, Smith-Jones P, et al. Targeting metastatic prostate cancer with radiolabeled monoclonal antibody J591 to the extracellular domain of prostate-specific membrane antigen. J Urol. 2003;170:1717–1721. doi: 10.1097/01.ju.0000091655.77601.0c. - DOI - PubMed
-
- Pinto JT, Suffoletto BP, Berzin TM, Qiao CH, Lin S, Tong WP, et al. Prostate-specific membrane antigen: a novel folate hydrolase in human prostatic carcinoma cells. Clin Cancer Res. 1996;2:1445–1451. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
