

Homozygous boricua TBCK mutation causes neurodegeneration and aberrant autophagy
- PMID: 29283439
- PMCID: PMC5876123
- DOI: 10.1002/ana.25130
Homozygous boricua TBCK mutation causes neurodegeneration and aberrant autophagy
Abstract
Objective: Autosomal-recessive mutations in TBCK cause intellectual disability of variable severity. Although the physiological function of TBCK remains unclear, loss-of-function mutations are associated with inhibition of mechanistic target of rapamycin complex 1 (mTORC1) signaling. Given that mTORC1 signaling is known to regulate autophagy, we hypothesized that TBCK-encephalopathy patients with a neurodegenerative course have defects in autophagic-lysosomal dysfunction.
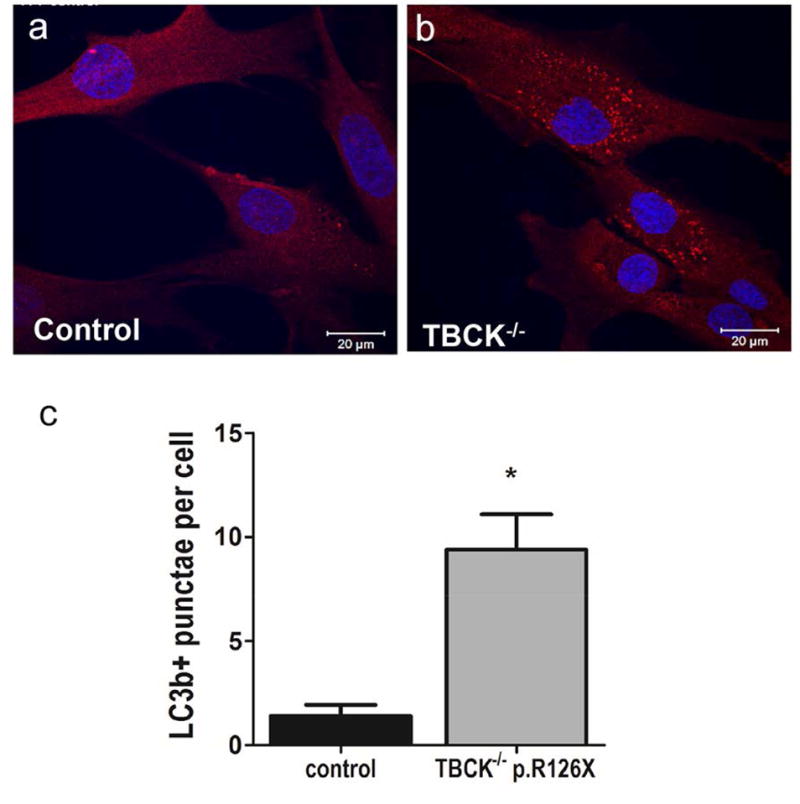
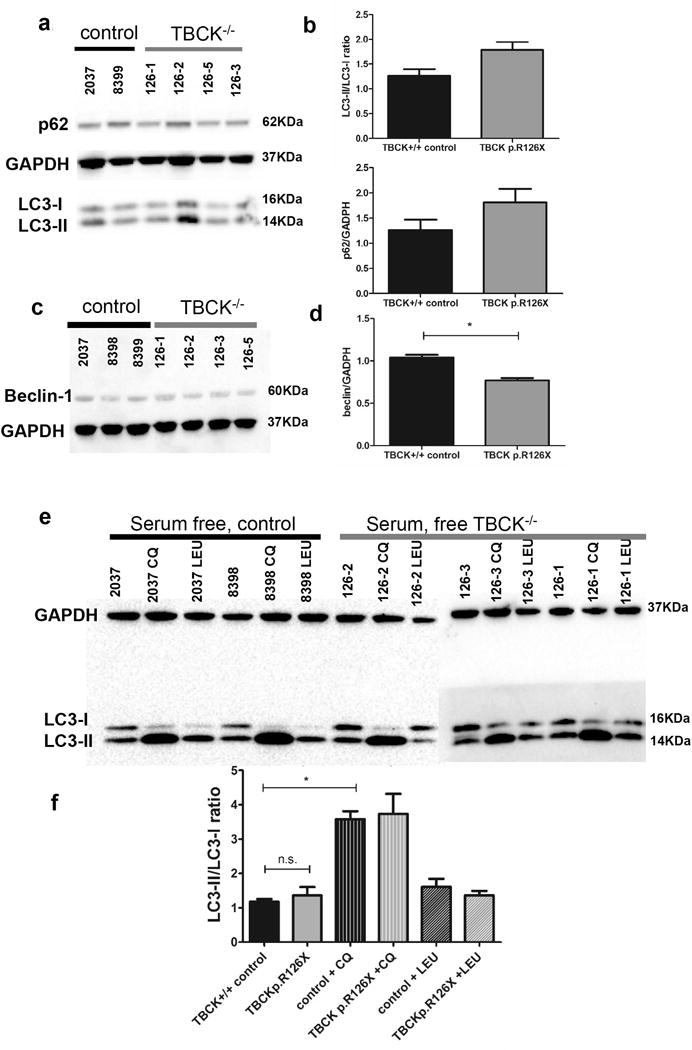
Methods: Children (n = 8) of Puerto Rican (Boricua) descent affected with homozygous TBCK p.R126X mutations underwent extensive neurological phenotyping and neurophysiological studies. We quantified autophagosome content in TBCK-/- patient-derived fibroblasts by immunostaining and assayed autophagic markers by western assay. Free sialylated oligosaccharide profiles were assayed in patient's urine and fibroblasts.
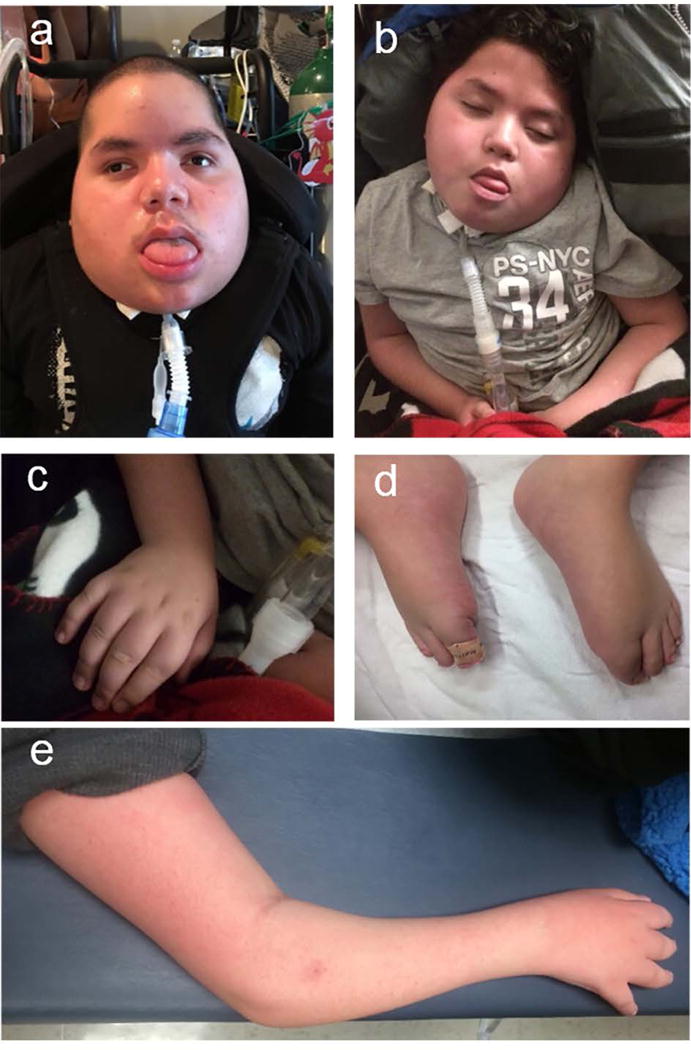
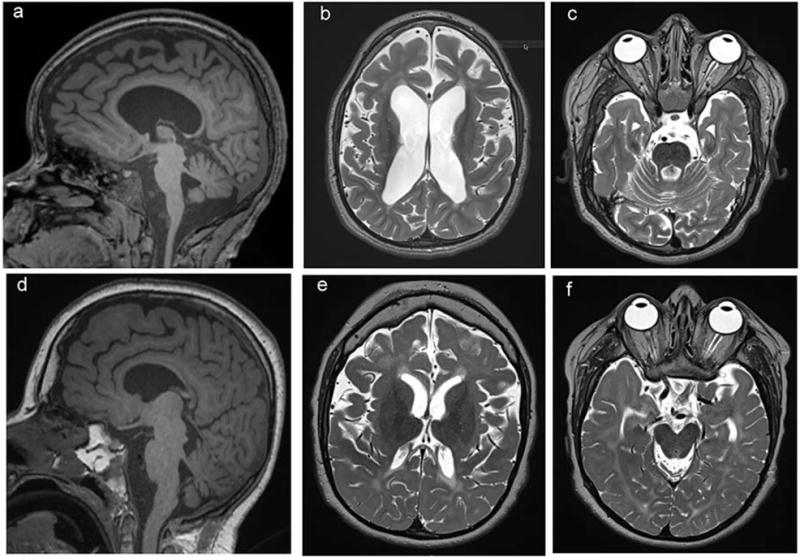
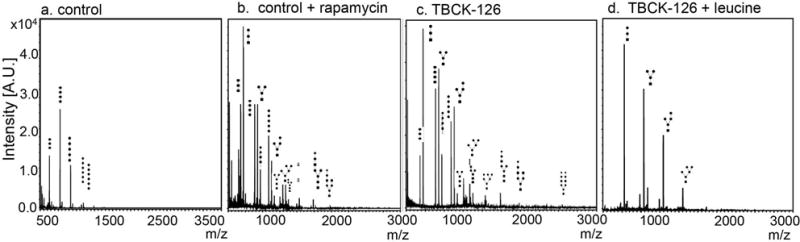
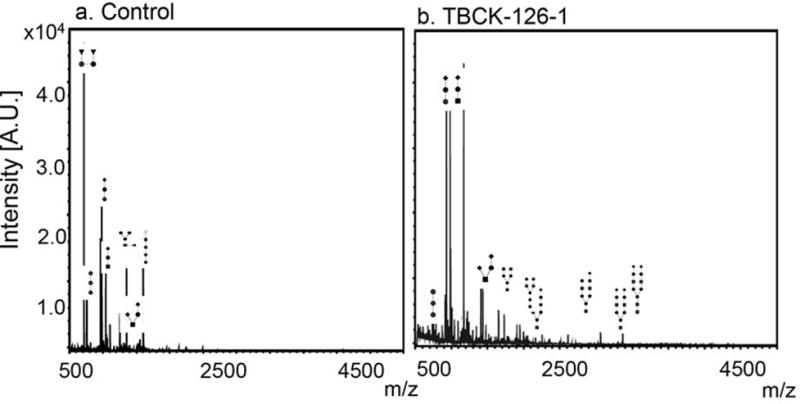
Results: The neurological phenotype of children with TBCK p.R126X mutations, which we call TBCK-encephaloneuronopathy (TBCKE), include congenital hypotonia, progressive motor neuronopathy, leukoencephalopathy, and epilepsy. Systemic features include coarse facies, dyslipidemia, and osteoporosis. TBCK-/- fibroblasts in vitro exhibit increased numbers of LC3+ autophagosomes and increased autophagic flux by immunoblots. Free oligosaccharide profiles in fibroblasts and urine of TBCKE patients differ from control fibroblasts and are ameliorated by treatment with the mTORC1 activator leucine.
Interpretation: TBCKE is a clinically distinguishable syndrome with progressive central and peripheral nervous system dysfunction, consistently observed in patients with the p.R126X mutation. We provide evidence that inappropriate autophagy in the absence of cellular stressors may play a role in this disorder, and that mTORC1 activation may ameliorate the autophagic-lysosomal system dysfunction. Free oligosaccharide profiles could serve as a novel biomarker for this disorder as well as a tool to evaluate potential therapeutic interventions. Ann Neurol 2018;83:153-165.
© 2017 American Neurological Association.
Conflict of interest statement
Nothing to disclose.
Figures
References
-
- Mandel H, Khayat M, Chervinsky E, Elpeleg O, Shalev S. TBCK-related intellectual disability syndrome: Case study of two patients. Am J Med Genet A. 2017 Feb;173(2):491–4. - PubMed
-
- Hartley T, Wagner JD, Warman-Chardon J, et al. Whole-exome sequencing is a valuable diagnostic tool for inherited peripheral neuropathies: outcomes from a cohort of 50 families. Clin Genet. 2017 Jul 14; - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
