

Interventions for Preventing Unintended, Rapid Repeat Pregnancy Among Adolescents: A Review of the Evidence and Lessons From High-Quality Evaluations
- PMID: 29284694
- PMCID: PMC5752603
- DOI: 10.9745/GHSP-D-17-00131
Interventions for Preventing Unintended, Rapid Repeat Pregnancy Among Adolescents: A Review of the Evidence and Lessons From High-Quality Evaluations
Abstract
Background: In 2017, of the 22.5 million parenting adolescents (ages 15-19) in 60 countries, approximately 4.1 million gave birth to a second or higher-order child. Adolescent pregnancy in general, and rapid repeat pregnancies specifically, expose young mothers and their children to multiple health and socioeconomic risks. The purpose of this article is to review the impact of interventions designed to prevent unintended, rapid repeat pregnancies among adolescents, including those aimed at changing norms to postpone "intended" closely spaced pregnancies to promote healthy spacing.
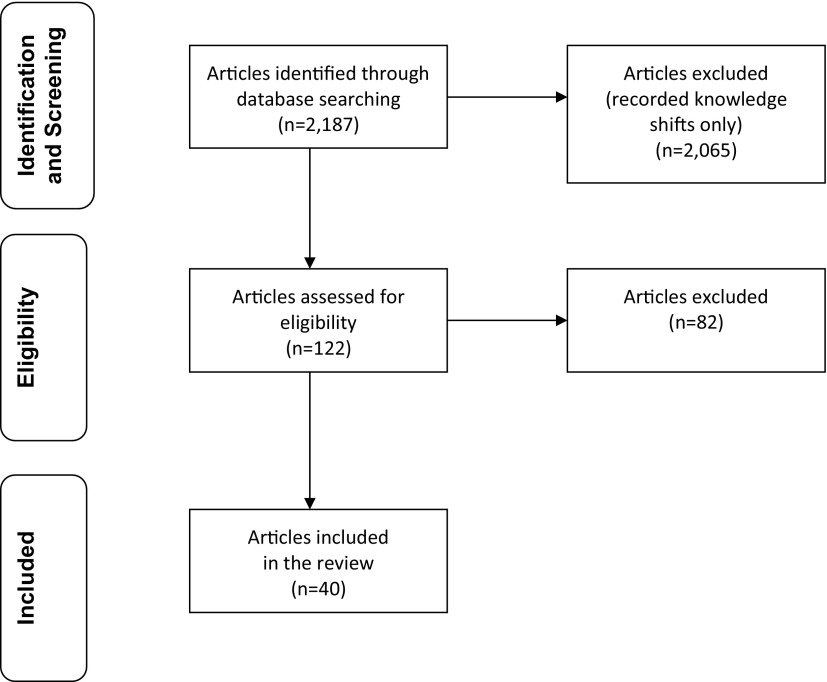
Methods: We searched PubMed and other databases for evaluations of interventions published in English from 1990 through 2016. We included evaluations that assessed a programmatic intervention specifically designed to prevent rapid repeat pregnancy (occurring less than 24 months after the index birth) or birth (occurring less than 33 months after the index birth), or that reported on contraceptive continuation for at least 2 years. We first assessed the quality of the evaluations, then ranked the interventions based on the quality of the evaluation and the level of impact on repeat pregnancy or birth (statistically significant impact, positive trends but not statistically significant, or no impact) to identify the most effective interventions. Finally, we extracted program design and implementation lessons from the interventions included in the high-quality evaluations.
Results: Our search identified 2,187 articles, of which 40 evaluations met the inclusion criteria (24=high quality, 14=moderate quality, 2=less rigorous). We found 14 high-quality evaluations in which the intervention achieved a statistically significant impact on repeat pregnancy or birth. These interventions fell into 5 broad categories: (1) contraceptive services and information, with proactive monitoring of contraceptive use and outreach to families; (2) postpartum contraceptive counseling and services provided soon after delivery; (3) activities that help adolescents improve planning skills, including preparing contraceptive plans; (4) social and behavioral change activities that help adolescents understand the role contraception can play in determining positive life outcomes, and the implications of their reproductive health decisions for their future; and (5) activities that provide mentoring, goal setting, and motivation.
Conclusion: Effective interventions that prevent rapid adolescent childbearing link clinical contraceptive services with non-clinical activities that build planning skills, enhance understanding of the role that contraceptives can play in determining positive life outcomes, and provide mentoring and goal setting. Recognizing potentially synergistic effects, we recommend testing various combinations of these interventions, with access to contraception as the foundational activity.
© Norton et al.
Figures

References
-
- Adolescence: a period needing special attention. Age--not the whole story. World Health Organization website. http://apps.who.int/adolescent/second-decade/section2/page2/age-not-the-... Accessed December 18, 2017.
-
- Neal S, Matthews Z, Frost M, Fogstad H, Camacho A, Laski L. Childbearing in adolescents aged 12-15 years in low resource countries: a neglected issue. New estimates from demographic and household surveys in 42 countries. Acta Obstet Gynecol Scand. 2012;91(9):1114–1118. 10.1111/j.1600-0412.2012.01467.x. - DOI - PubMed
-
- Ross JA, Winfrey WL. Contraceptive use, intention to use, and unmet need in the extended postpartum period. Int Fam Plan Perspect. 2001;27(1):20–27. https://www.guttmacher.org/journals/ipsrh/2001/03/contraceptive-use-inte... Accessed December 12, 2017.
-
- Hoffman S, Maynard R. Kids having kids: economic costs and social consequences of teen pregnancy. Washington, DC: The Urban Institute; 2008.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous