

Intracranial Ewing sarcoma: four pediatric examples
- PMID: 29285586
- PMCID: PMC5808087
- DOI: 10.1007/s00381-017-3684-7
Intracranial Ewing sarcoma: four pediatric examples
Abstract
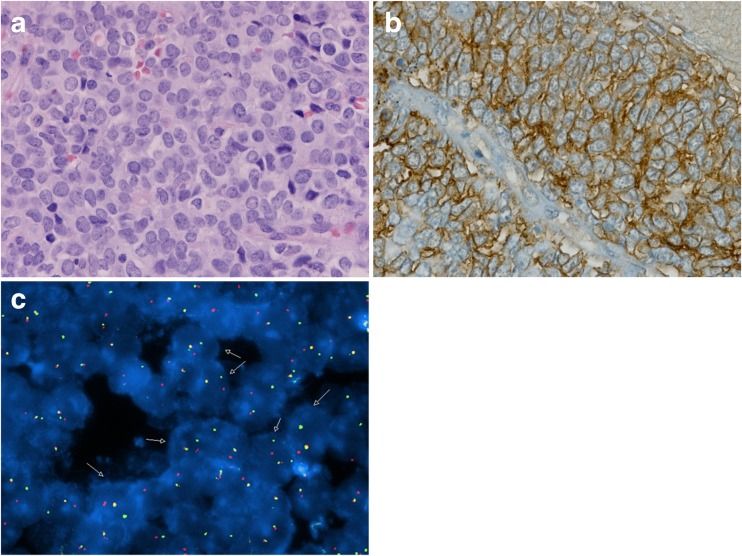
Background: Ewing sarcoma typically arises in bone and is unrelated to intraparenchymal small blue cell embryonal central nervous system (CNS) tumors previously designated primitive neuroectodermal tumors (PNETs). When the CNS is impacted, it is usually secondary to local extension from either the epidural space, skull, or intracranial or spinal metastases. Primary examples within the cranial vault are rare, usually dural-based, and are largely case reports in the literature. We detail four pediatric patients with solitary, primary intracranial Ewing sarcoma, all manifesting the archetypal EWRS1 gene rearrangement that confirms diagnosis.
Procedure: Neurosurgical Department records, spanning 21 years (1995-2016), were reviewed to identify patients. Demographics, clinical history, pathological/genetic features, and clinical course were retrieved from the medical record and personal files of the authors.
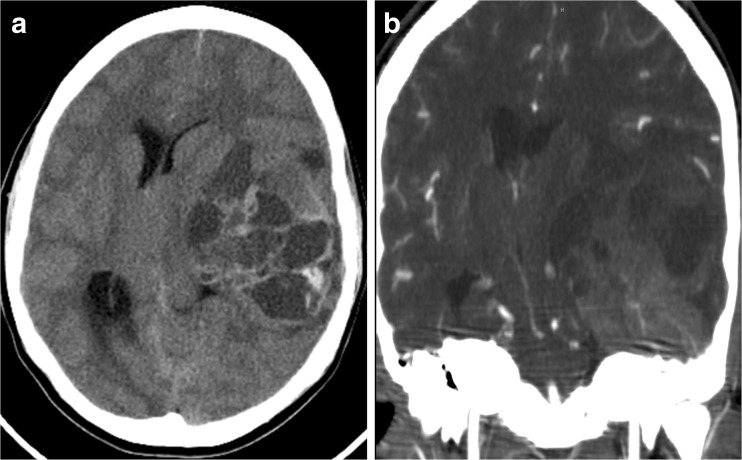
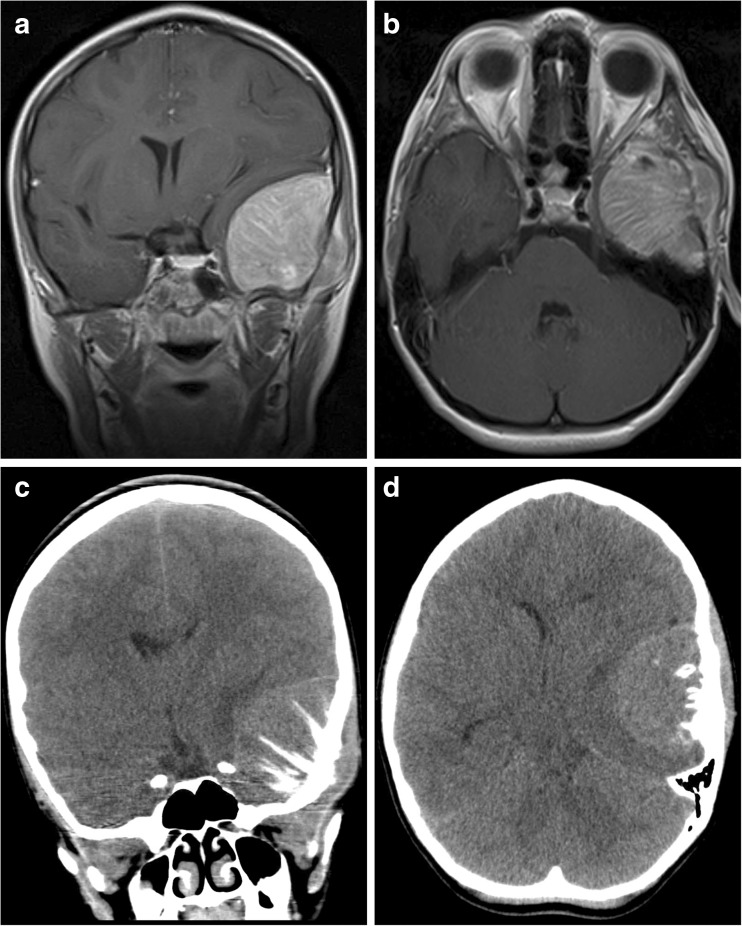
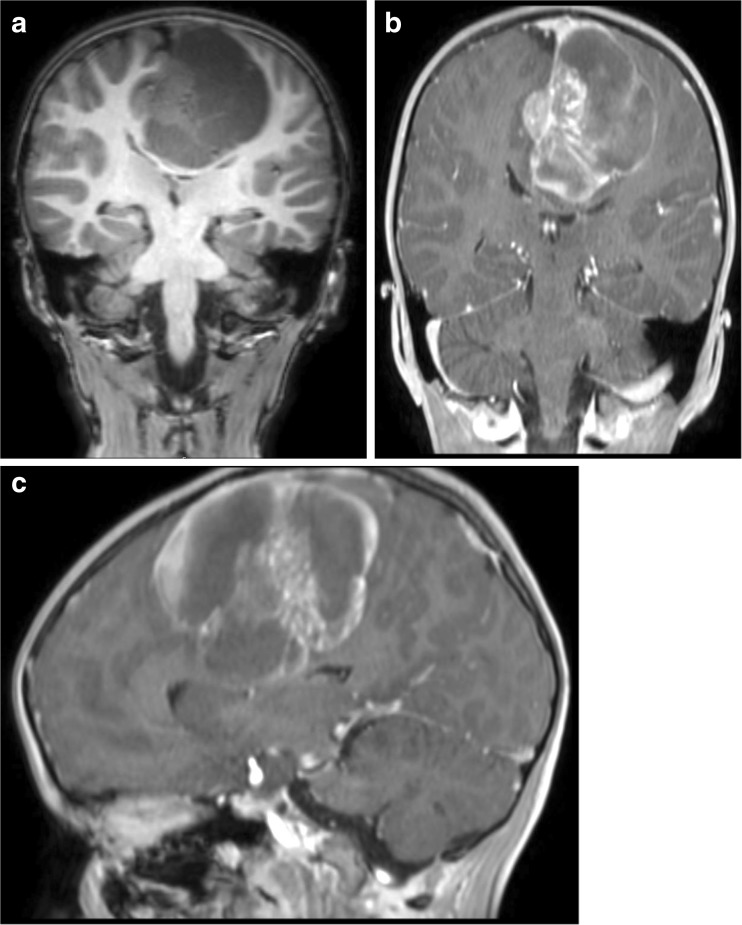
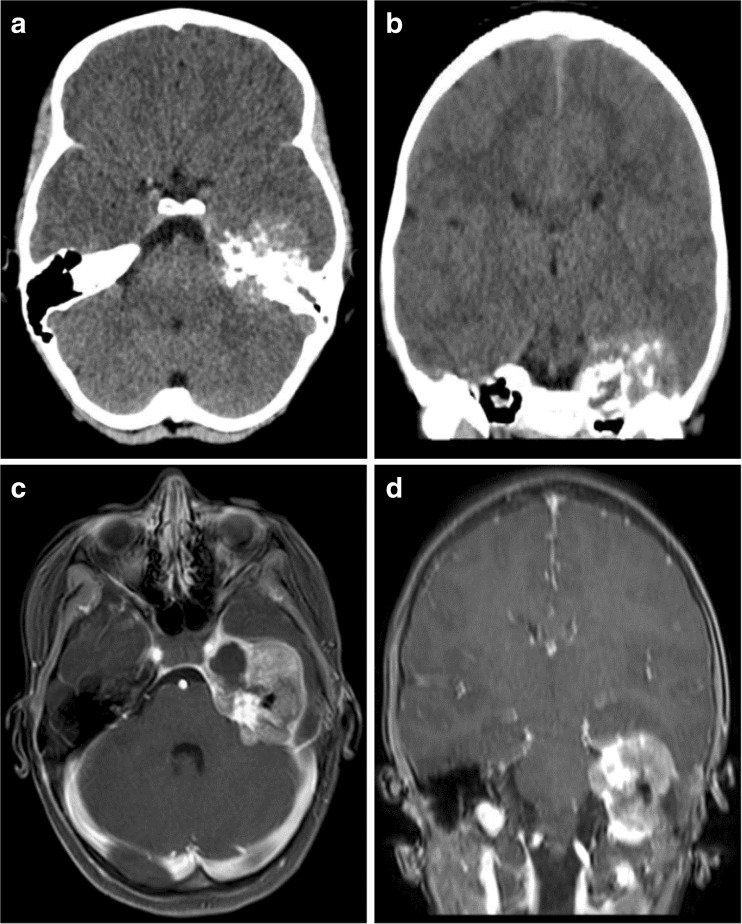
Results: Four patients, one male and three females, age 5 to 16 years, were identified. One presented in extremis from a large lesion, two with soft tissue masses, and the fourth as an incidental finding after being involved in a motor vehicle collision. Three had clear bony involvement: a 10-year-old girl with a large left temporal lesion had clear origin in the skull, with spiculated calcified striations throughout the mass; a 9-year-old girl presented with a bony left petrous apex mass; and a 16-year-old girl presented with a left temporal mass with extension to the dura and underlying bone erosion. Only the 5-year-old boy had a large left frontoparietal mass traversing the falx with no bony contact. All four tumors manifested the diagnostic EWSR1 mutation and were treated with an Ewing sarcoma regimen. Outcomes were variable, with one patient showing progressive metastatic disease and death 3 years after presentation, one patient with disease-free survival 10.5 years after completion of therapy, and one alive and well at the completion of therapy 1 year after diagnosis. One patient completed therapy recently with post-therapy scans showing no evidence of disease.
Conclusion: Testing for the EWSR1 mutation confirms the diagnosis of Ewing sarcoma and excludes other types of embryonal CNS tumors. Long-term disease-free survival is possible with adherence to the appropriate therapeutic regimen after gross surgical resection.
Keywords: EWSR1 gene; Intracranial Ewing sarcoma; PNET; Pediatric brain tumor.
Conflict of interest statement
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Figures
References
-
- Cancer Facts & Figures 2016. American Cancer Society
-
- Gurney J, Swensen A, Bulterys M: Malignant bone tumors. In: Cancer incidence and survival among children and adolescents: United States SEER program 1975-1995. NCI, SEER Program, 1999
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
