

An Interpretable Machine Learning Model for Accurate Prediction of Sepsis in the ICU
- PMID: 29286945
- PMCID: PMC5851825
- DOI: 10.1097/CCM.0000000000002936
An Interpretable Machine Learning Model for Accurate Prediction of Sepsis in the ICU
Abstract
Objectives: Sepsis is among the leading causes of morbidity, mortality, and cost overruns in critically ill patients. Early intervention with antibiotics improves survival in septic patients. However, no clinically validated system exists for real-time prediction of sepsis onset. We aimed to develop and validate an Artificial Intelligence Sepsis Expert algorithm for early prediction of sepsis.
Design: Observational cohort study.
Setting: Academic medical center from January 2013 to December 2015.
Patients: Over 31,000 admissions to the ICUs at two Emory University hospitals (development cohort), in addition to over 52,000 ICU patients from the publicly available Medical Information Mart for Intensive Care-III ICU database (validation cohort). Patients who met the Third International Consensus Definitions for Sepsis (Sepsis-3) prior to or within 4 hours of their ICU admission were excluded, resulting in roughly 27,000 and 42,000 patients within our development and validation cohorts, respectively.
Interventions: None.
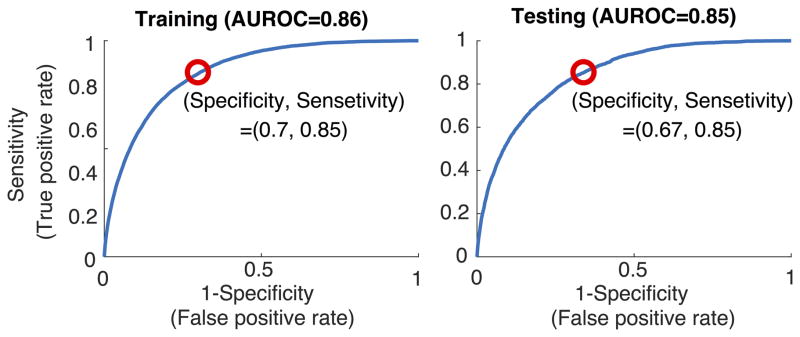
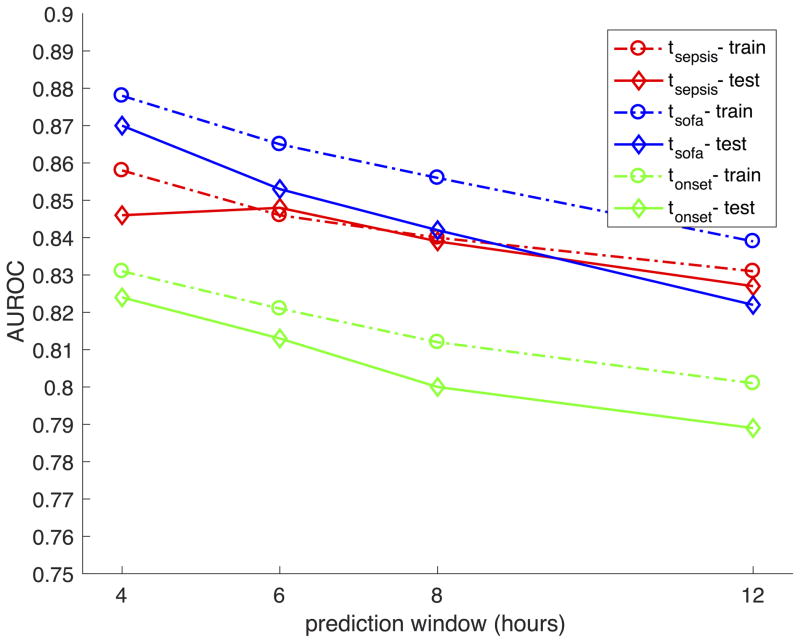
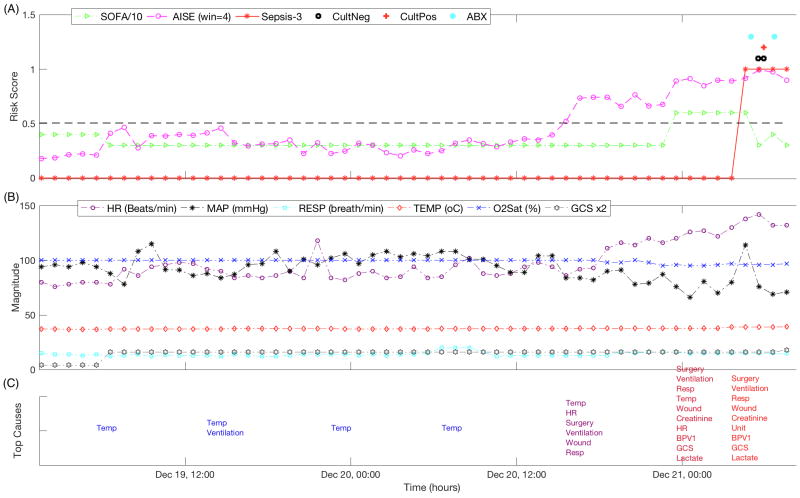
Measurements and main results: High-resolution vital signs time series and electronic medical record data were extracted. A set of 65 features (variables) were calculated on hourly basis and passed to the Artificial Intelligence Sepsis Expert algorithm to predict onset of sepsis in the proceeding T hours (where T = 12, 8, 6, or 4). Artificial Intelligence Sepsis Expert was used to predict onset of sepsis in the proceeding T hours and to produce a list of the most significant contributing factors. For the 12-, 8-, 6-, and 4-hour ahead prediction of sepsis, Artificial Intelligence Sepsis Expert achieved area under the receiver operating characteristic in the range of 0.83-0.85. Performance of the Artificial Intelligence Sepsis Expert on the development and validation cohorts was indistinguishable.
Conclusions: Using data available in the ICU in real-time, Artificial Intelligence Sepsis Expert can accurately predict the onset of sepsis in an ICU patient 4-12 hours prior to clinical recognition. A prospective study is necessary to determine the clinical utility of the proposed sepsis prediction model.
Conflict of interest statement
The remaining authors have disclosed that they do not have any remaining conflicts of interest. The opinions or assertions contained herein are the private ones of the author/speaker and are not to be construed as official or reflecting the views of the Department of Defense, the Uniformed Services University of the Health Sciences or any other agency of the U.S. Government.
Figures
References
-
- Angus DC, Linde-Zwirble WT, Lidicker J, et al. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29(7):1303–10. - PubMed
-
- Arise AAM Committee. The outcome of patients with sepsis and septic shock presenting to emergency departments in Australia and New Zealand. Crit Care Resusc. 2007;9(1):8–18. - PubMed
-
- Martin GS, Mannino DM, Eaton S, et al. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med. 2003;348(16):1546–54. - PubMed
-
- Stoller J, Halpin L, Weis M, et al. Epidemiology of severe sepsis: 2008–2012. J Crit Care. 2016;31(1):58–62. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
