

A diagnostic and epidemiologic investigation of acute febrile illness (AFI) in Kilombero, Tanzania
- PMID: 29287070
- PMCID: PMC5747442
- DOI: 10.1371/journal.pone.0189712
A diagnostic and epidemiologic investigation of acute febrile illness (AFI) in Kilombero, Tanzania
Abstract
Introduction: In low-resource settings, empiric case management of febrile illness is routine as a result of limited access to laboratory diagnostics. The use of comprehensive fever syndromic surveillance, with enhanced clinical microbiology, advanced diagnostics and more robust epidemiologic investigation, could enable healthcare providers to offer a differential diagnosis of fever syndrome and more appropriate care and treatment.
Methods: We conducted a year-long exploratory study of fever syndrome among patients ≥ 1 year if age, presenting to clinical settings with an axillary temperature of ≥37.5°C and symptomatic onset of ≤5 days. Blood and naso-pharyngeal/oral-pharyngeal (NP/OP) specimens were collected and analyzed, respectively, using AFI and respiratory TaqMan Array Cards (TAC) for multi-pathogen detection of 57 potential causative agents. Furthermore, we examined numerous epidemiologic correlates of febrile illness, and conducted demographic, clinical, and behavioral domain-specific multivariate regression to statistically establish associations with agent detection.
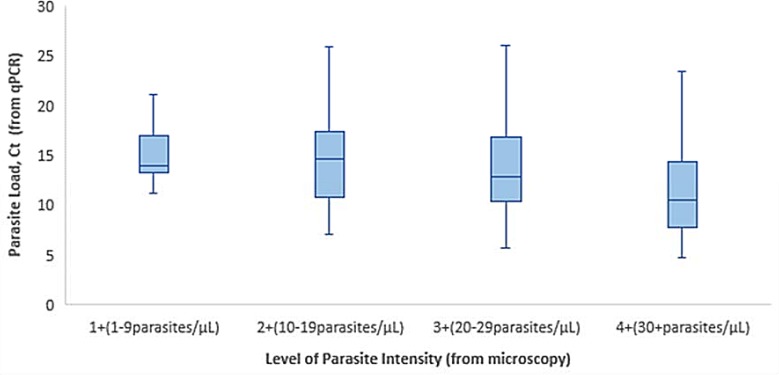
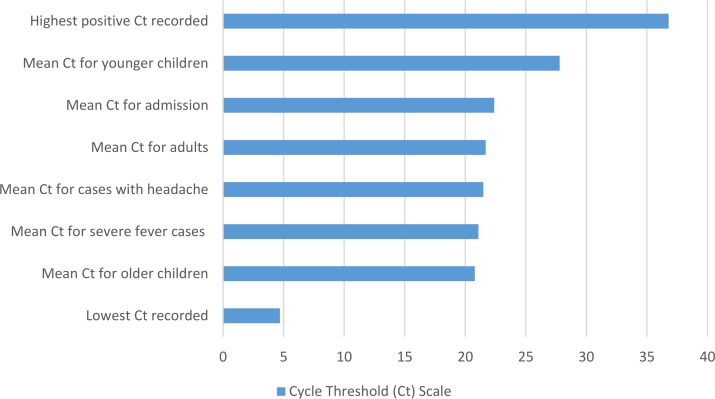
Results: From 15 September 2014-13 September 2015, 1007 febrile patients were enrolled, and 997 contributed an epidemiologic survey, including: 14% (n = 139) 1<5yrs, 19% (n = 186) 5-14yrs, and 67% (n = 672) ≥15yrs. AFI TAC and respiratory TAC were performed on 842 whole blood specimens and 385 NP/OP specimens, respectively. Of the 57 agents surveyed, Plasmodium was the most common agent detected. AFI TAC detected nucleic acid for one or more of seven microbial agents in 49% of AFI blood samples, including: Plasmodium (47%), Leptospira (3%), Bartonella (1%), Salmonella enterica (1%), Coxiella burnetii (1%), Rickettsia (1%), and West Nile virus (1%). Respiratory TAC detected nucleic acid for 24 different microbial agents, including 12 viruses and 12 bacteria. The most common agents detected among our surveyed population were: Haemophilus influenzae (67%), Streptococcus pneumoniae (55%), Moraxella catarrhalis (39%), Staphylococcus aureus (37%), Pseudomonas aeruginosa (36%), Human Rhinovirus (25%), influenza A (24%), Klebsiella pneumoniae (14%), Enterovirus (15%) and group A Streptococcus (12%). Our epidemiologic investigation demonstrated both age and symptomatic presentation to be associated with a number of detected agents, including, but not limited to, influenza A and Plasmodium. Linear regression of fully-adjusted mean cycle threshold (Ct) values for Plasmodium also identified statistically significant lower mean Ct values for older children (20.8), patients presenting with severe fever (21.1) and headache (21.5), as well as patients admitted for in-patient care and treatment (22.4).
Conclusions: This study is the first to employ two syndromic TaqMan Array Cards for the simultaneous survey of 57 different organisms to better characterize the type and prevalence of detected agents among febrile patients. Additionally, we provide an analysis of the association between adjusted mean Ct values for Plasmodium and key clinical and demographic variables, which may further inform clinical decision-making based upon intensity of infection, as observed across endemic settings of sub-Saharan Africa.
Conflict of interest statement
Figures
References
-
- Crump JA. Typhoid Fever and the challenge of nonmalaria febrile illness in sub-saharan Africa. Clin Infect Dis 2012. April;54(8):1107–1109. doi: 10.1093/cid/cis024 - DOI - PubMed
-
- Reddy EA, Shaw AV, Crump JA. Community-acquired bloodstream infections in Africa: a systematic review and meta-analysis. Lancet Infect Dis 2010. June;10(6):417–432. doi: 10.1016/S1473-3099(10)70072-4 - DOI - PMC - PubMed
-
- O’Meara WP, Mangeni JN, Steketee R, Greenwood B. Changes in the burden of malaria in sub-Saharan Africa. Lancet Infect Dis 2010; 10:545–555. doi: 10.1016/S1473-3099(10)70096-7 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
