

Complete remission of hypertension in a hemodialysis patient after adrenalectomy for primary aldosteronism and renal transplantation
- PMID: 29288290
- PMCID: PMC5886930
- DOI: 10.1007/s13730-017-0299-5
Complete remission of hypertension in a hemodialysis patient after adrenalectomy for primary aldosteronism and renal transplantation
Abstract
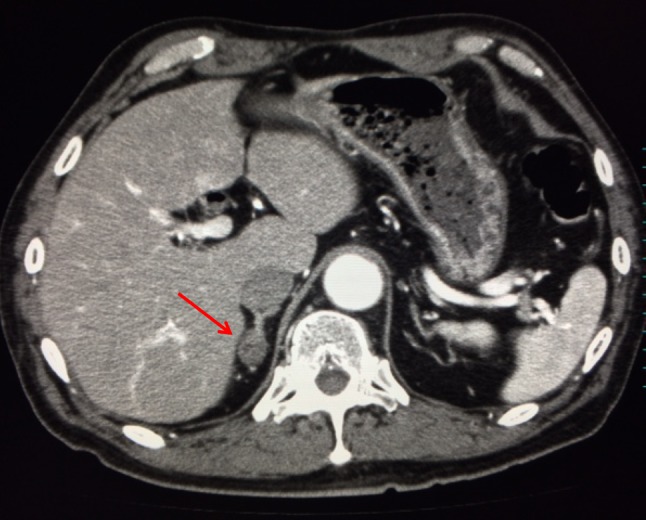
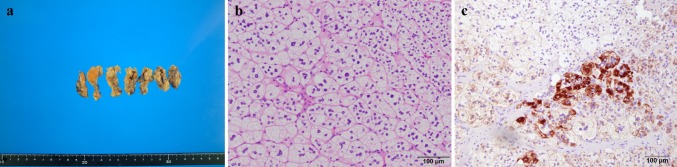
A 64-year-old man was admitted to our hospital for the hormonal evaluation of a right adrenal adenoma. He had been diagnosed with severe proteinuria and hypertension, and antihypertensive treatment was started at the age of 60. His renal function gradually declined, and hemodialysis was begun at the age of 64. Since his blood pressure was uncontrollable and resistant to antihypertensive treatment, an endocrinological examination was performed for an incidental right adrenal mass detected by computed tomography. The results of screening, including captopril challenge and an adrenocorticotropin stimulation test for primary aldosteronism, and adrenal venous sampling suggested excessive aldosterone secretion from the right adrenal gland. Adrenalectomy was performed; his blood pressure decreased and became well-controlled with a reduced antihypertensive regimen. Furthermore, he received renal transplantation which resulted in normalization of his serum potassium level, improvement of renal function and hormonal levels such as plasma renin activity and aldosterone concentration, and satisfactory blood pressure without any antihypertensive medications. This case is extremely important to demonstrate the effects of adrenalectomy for primary aldosteronism in a hemodialysis patient. It is possible that adrenalectomy may be a useful treatment for primary aldosteronism even in patients undergoing hemodialysis. Careful long-term follow-up of our case and investigations of the efficacy of adrenalectomy in similar cases are needed to address this issue.
Keywords: Aldosterone; Blood pressure; End-stage renal disease; Renin; Surgery.
Conflict of interest statement
Conflict of interest
All the authors have declared no competing interest.
Human and animal rights
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
Informed consent was obtained from all the individual participants included in the study.
Figures

References
-
- Funder JW, Carey RM, Mantero F, Murad MH, Reincke M, Shibata H, Stowasser M, Young WF., Jr The management of primary aldosteronism: case detection, diagnosis, and treatment: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2016;101:1889–1916. doi: 10.1210/jc.2015-4061. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
