

Laparoscopic surgery for locally advanced T4 colon cancer: the long-term outcomes and prognostic factors
- PMID: 29288349
- PMCID: PMC5880863
- DOI: 10.1007/s00595-017-1621-8
Laparoscopic surgery for locally advanced T4 colon cancer: the long-term outcomes and prognostic factors
Abstract
Purpose: For locally advanced pathological T4 (pT4) colon cancer, the safety and feasibility of laparoscopic procedures remain controversial. Therefore, this study aimed to assess short-term and long-term outcomes and to identify the prognostic factors in laparoscopic surgery for pT4 colon cancer.
Methods: The study group included 130 patients who underwent laparoscopic radical resection for pT4 colon and rectosigmoid cancer from January 2004 through December 2012. The short-term outcomes, long-term outcomes, and prognostic factors in pT4 colon cancer were analyzed.
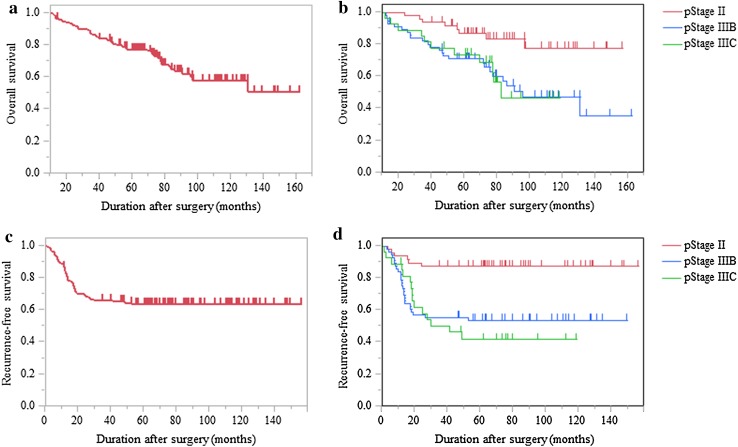
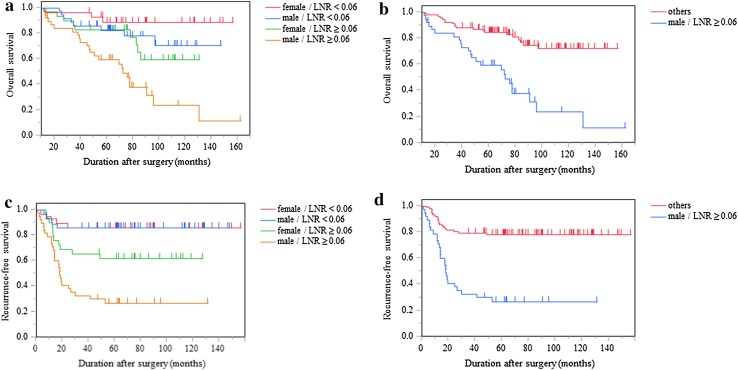
Results: The median operative time was 205 min, with a median blood loss of 10 ml. The conversion rate was 3.8%, and 13 patients (10.0%) had postoperative complications. The radial resection margin was positive in 1 patient (0.8%). The median follow-up time was 73 months. The 5-year overall survival (OS) and recurrence-free survival (RFS) were 77.2 and 63.5%, respectively. On a multivariate analysis, a male sex [hazard ratio (HR) 3.09, p < 0.001], lymph node ratio ≥ 0.06 (HR 2.35, p = 0.021), tumor diameter < 38 mm (HR 2.57, p = 0.007), and right-sided colon cancer (HR 2.11, p = 0.047) were significantly related to a poor OS.
Conclusions: These results suggest that laparoscopic surgery for pT4 colon cancer is safe and feasible, and the oncological outcomes are acceptable. Based on the present findings, select patients with locally advanced colon cancer should not be excluded from laparoscopic surgery.
Keywords: Colorectal cancer; Laparoscopic surgery; Long-term outcomes; Prognostic factors; T4 colon cancer.
Conflict of interest statement
Takahiro Yamanashi and the other co-authors have no conflicts of interest.
Figures
References
-
- Guillou PJ, Quirke P, Thorpe H, Walker J, Jayne DG, Smith AMH, et al. Short-term endpoints of conventional versus laparoscopic-assisted surgery in patients with colorectal cancer (MRC CLASICC trial): multicentre, randomised controlled trial. Lancet. 2005;365:1718–1726. doi: 10.1016/S0140-6736(05)66545-2. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
