

PanCancer insights from The Cancer Genome Atlas: the pathologist's perspective
- PMID: 29288495
- PMCID: PMC6240356
- DOI: 10.1002/path.5028
PanCancer insights from The Cancer Genome Atlas: the pathologist's perspective
Abstract
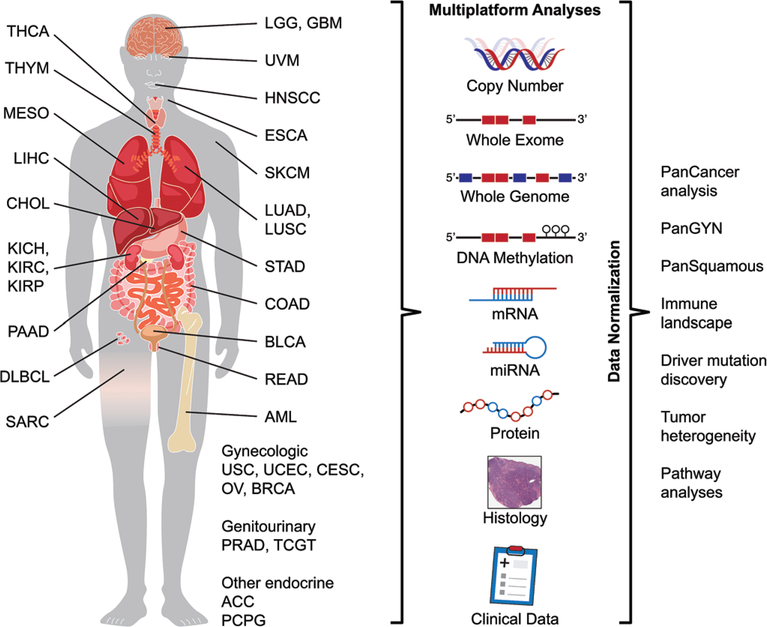
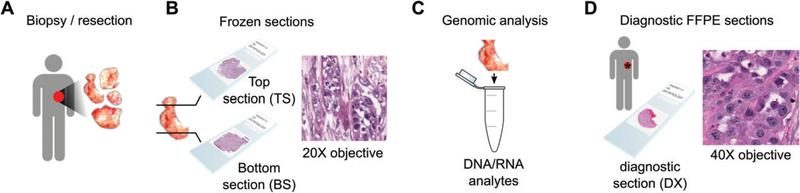
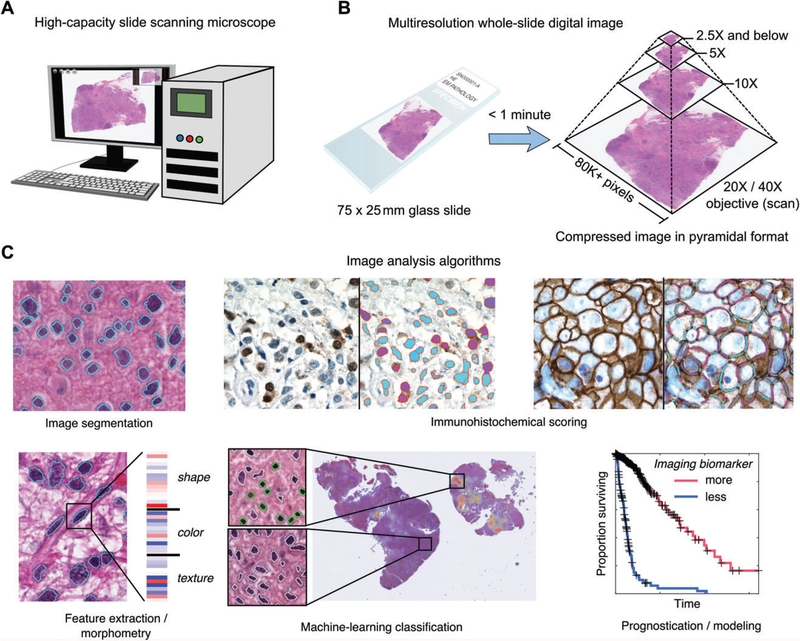
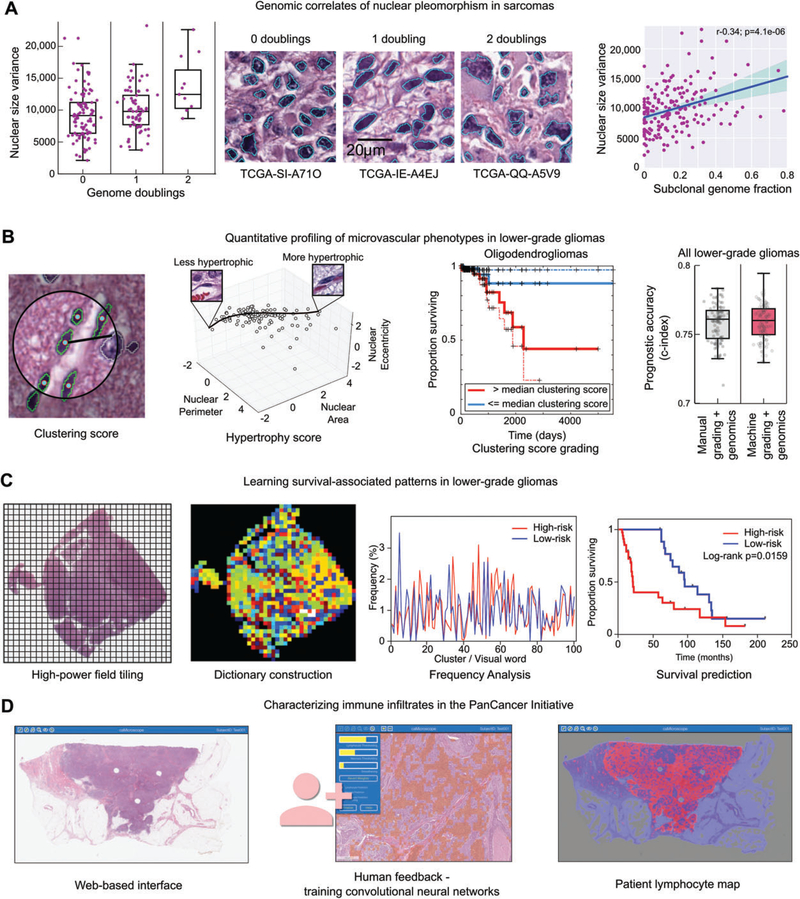
The Cancer Genome Atlas (TCGA) represents one of several international consortia dedicated to performing comprehensive genomic and epigenomic analyses of selected tumour types to advance our understanding of disease and provide an open-access resource for worldwide cancer research. Thirty-three tumour types (selected by histology or tissue of origin, to include both common and rare diseases), comprising >11 000 specimens, were subjected to DNA sequencing, copy number and methylation analysis, and transcriptomic, proteomic and histological evaluation. Each cancer type was analysed individually to identify tissue-specific alterations, and make correlations across different molecular platforms. The final dataset was then normalized and combined for the PanCancer Initiative, which seeks to identify commonalities across different cancer types or cells of origin/lineage, or within anatomically or morphologically related groups. An important resource generated along with the rich molecular studies is an extensive digital pathology slide archive, composed of frozen section tissue directly related to the tissues analysed as part of TCGA, and representative formalin-fixed paraffin-embedded, haematoxylin and eosin (H&E)-stained diagnostic slides. These H&E image resources have primarily been used to verify diagnoses and histological subtypes with some limited extraction of standard pathological variables such as mitotic activity, grade, and lymphocytic infiltrates. Largely overlooked is the richness of these scanned images for more sophisticated feature extraction approaches coupled with machine learning, and ultimately correlation with molecular features and clinical endpoints. Here, we document initial attempts to exploit TCGA imaging archives, and describe some of the tools, and the rapidly evolving image analysis/feature extraction landscape. Our hope is to inform, and ultimately inspire and challenge, the pathology and cancer research communities to exploit these imaging resources so that the full potential of this integral platform of TCGA can be used to complement and enhance the insightful integrated analyses from the genomic and epigenomic platforms. Copyright © 2017 Pathological Society of Great Britain and Ireland. Published by John Wiley & Sons, Ltd.
Keywords: PanCancer; TCGA; The Cancer Genome Atlas; computational histology; digital pathology; genomics; image analysis.
Copyright © 2017 Pathological Society of Great Britain and Ireland. Published by John Wiley & Sons, Ltd.
Conflict of interest statement
No conflicts of interest were declared.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
