

Abnormalities of laboratory coagulation tests versus clinically evident coagulopathic bleeding: results from the prehospital resuscitation on helicopters study (PROHS)
- PMID: 29289392
- PMCID: PMC5903880
- DOI: 10.1016/j.surg.2017.10.050
Abnormalities of laboratory coagulation tests versus clinically evident coagulopathic bleeding: results from the prehospital resuscitation on helicopters study (PROHS)
Abstract
Background: Laboratory-based evidence of coagulopathy (LC) is observed in 25-35% of trauma patients, but clinically-evident coagulopathy (CC) is not well described.
Methods: Prospective observational study of adult trauma patients transported by helicopter from the scene to nine Level 1 trauma centers in 2015. Patients meeting predefined highest-risk criteria were divided into CC+ (predefined as surgeon-confirmed bleeding from uninjured sites or injured sites not controllable by sutures) or CC-. We used a mixed-effects, Poisson regression with robust error variance to test the hypothesis that abnormalities on rapid thrombelastography (r-TEG) and international normalized ratio (INR) were independently associated with CC+.
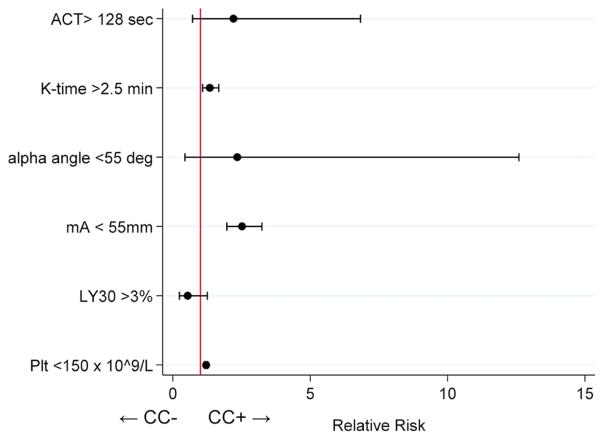
Results: Of 1,019 highest-risk patients, CC+ (n=41, 4%) were more severely injured (median ISS 32 vs 17), had evidence of LC on r-TEG and INR, received more transfused blood products at 4 hours (37 vs 0 units), and had greater 30-day mortality (59% vs 12%) than CC- (n=978, 96%). The overall incidence of LC was 39%. 30-day mortality was 22% vs 9% in those with and without LC. In two separate models, r-TEG K-time >2.5 min (RR 1.3, 95% CI 1.1-1.7), r-TEG mA <55 mm (RR 2.5, 95% CI 2.0-3.2), platelet count <150 x 109/L (RR 1.2, 95% CI 1.1-1.3), and INR >1.5 (RR 5.4, 95% CI 1.8-16.3) were independently associated with CC+. A combined regression model was not generated because too few patients underwent both r-TEG and INR.
Conclusion: CC was rare compared to LC. CC was associated with poor outcomes and impairment of both clotting factor and platelet-mediated coagulation components.
Copyright © 2017 Elsevier Inc. All rights reserved.
Figures
References
-
- National Vital Statistics System, National Center for Health Statistics, Centers for Disease Control and Prevention. 10 Leading Causes of death by Age Group, United States—2013. Atlanta, GA: Office of Statistics and Programing, National Center for Injury Prevention and Control, Centers for Disease Control and Prevention; [Accessed December 30, 2016]. http://www.cdc.gov/injury/images/lc-charts/leading_causes_of_death_by_ag....
-
- Niles SE, McLaughlin DF, Perkins JG, Wade CE, Li Y, Spinella PC, Holcomb JB. Increased mortality associated with the early coagulopathy of trauma in combat casualties. J Trauma. 2008;64(6):1459–63. - PubMed
-
- Brohi K, Singh J, Heron M, Coats T. Acute traumatic coagulopathy. J Trauma. 2003;54(6):1127–30. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
