

Cystic Fibrosis Colorectal Cancer Screening Consensus Recommendations
- PMID: 29289528
- PMCID: PMC9675422
- DOI: 10.1053/j.gastro.2017.12.012
Cystic Fibrosis Colorectal Cancer Screening Consensus Recommendations
Abstract
Background & aims: Improved therapy has substantially increased survival of persons with cystic fibrosis (CF). But the risk of colorectal cancer (CRC) in adults with CF is 5-10 times greater compared to the general population, and 25-30 times greater in CF patients after an organ transplantation. To address this risk, the CF Foundation convened a multi-stakeholder task force to develop CRC screening recommendations.
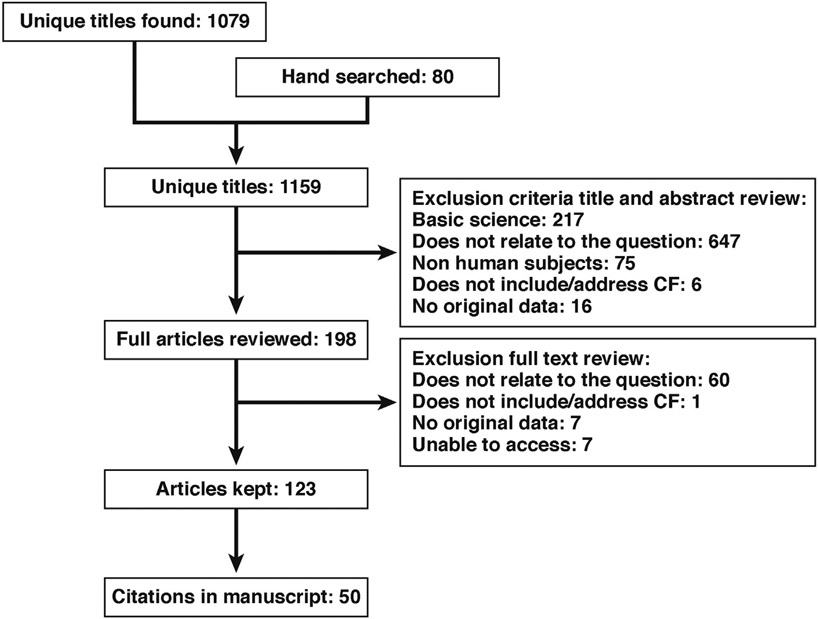
Methods: The 18-member task force consisted of experts including pulmonologists, gastroenterologists, a social worker, nurse coordinator, surgeon, epidemiologist, statistician, CF adult, and a parent. The committee comprised 3 workgroups: Cancer Risk, Transplant, and Procedure and Preparation. A guidelines specialist at the CF Foundation conducted an evidence synthesis February-March 2016 based on PubMed literature searches. Task force members conducted additional independent searches. A total of 1159 articles were retrieved. After initial screening, the committee read 198 articles in full and analyzed 123 articles to develop recommendation statements. An independent decision analysis evaluating the benefits of screening relative to harms and resources required was conducted by the Department of Public Health at Erasmus Medical Center, Netherlands using the Microsimulation Screening Analysis model from the Cancer Innervation and Surveillance Modeling Network. The task force included recommendation statements in the final guideline only if they reached an 80% acceptance threshold.
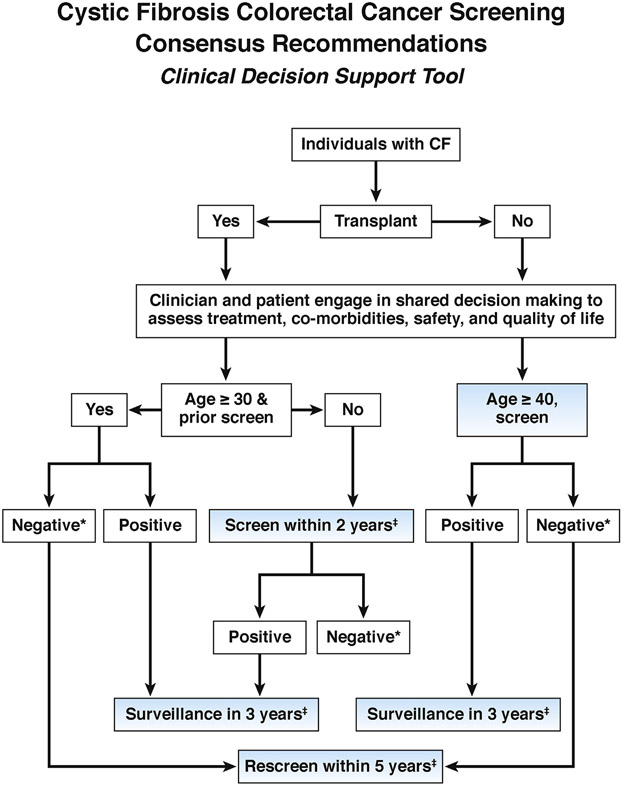
Results: The task force makes 10 CRC screening recommendations that emphasize shared, individualized decision-making and familiarity with CF-specific gastrointestinal challenges. We recommend colonoscopy as the preferred screening method, initiation of screening at age 40 years, 5-year re-screening and 3-year surveillance intervals (unless shorter interval is indicated by individual findings), and a CF-specific intensive bowel preparation. Organ transplant recipients with CF should initiate CRC screening at age 30 years within 2 years of the transplantation because of the additional risk for colon cancer associated with immunosuppression.
Conclusions: These recommendations aim to help CF adults, families, primary care physicians, gastroenterologists, and CF and transplantation centers address the issue of CRC screening. They differ from guidelines developed for the general population with respect to the recommended age of screening initiation, screening method, preparation, and the interval for repeat screening and surveillance.
Keywords: CFTR; Cancer; Colon; Colonoscopy; Cost-Effectiveness Analysis; Cystic Fibrosis; Intestine; Large Bowel; Recommendations; Rectum; Screening.
Copyright © 2018 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of interest
The authors disclose no conflicts.
Figures
Comment in
-
Cancer Risk in Patients With Cystic Fibrosis.Gastroenterology. 2018 Jun;154(8):2282-2283. doi: 10.1053/j.gastro.2018.02.040. Epub 2018 May 5. Gastroenterology. 2018. PMID: 29738750 No abstract available.
-
Reply.Gastroenterology. 2018 Jun;154(8):2283-2284. doi: 10.1053/j.gastro.2018.05.017. Epub 2018 May 8. Gastroenterology. 2018. PMID: 29750906 No abstract available.
References
-
- Cystic Fibrosis Foundation. Cystic Fibrosis Foundation Patient Registry 2015 Annual Data Report. Bethesda, MD: Cystic Fibrosis Foundation, 2016.
-
- Maisonneuve P, FitzSimmons SC, Neglia JP, Campbell PW 3rd, Lowenfels AB. Cancer risk in non-transplanted and transplanted cystic fibrosis patients: a 10-year study. J Natl Cancer Inst 2003;95:381–387. - PubMed
-
- Maisonneuve P, Marshall BC, Knapp EA, Lowenfels AB. Cancer risk in cystic fibrosis: a 20-year nationwide study from the United States. J Natl Cancer Inst 2013;105:122–129. - PubMed
-
- Neglia JP, FitzSimmons SC, Maisonneuve P, et al. The risk of cancer among patients with cystic fibrosis. Cystic Fibrosis and Cancer Study Group. N Engl J Med 1995;332:494–499. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
