

Cost-effectiveness of Drugs to Treat Relapsed/Refractory Multiple Myeloma in the United States
- PMID: 29290170
- PMCID: PMC10398323
- DOI: 10.18553/jmcp.2018.24.1.29
Cost-effectiveness of Drugs to Treat Relapsed/Refractory Multiple Myeloma in the United States
Abstract
Background: New 3-drug regimens have been developed and approved to treat multiple myeloma (MM). The absence of direct comparative data and the high cost of treatment support the need to assess the relative clinical and economic outcomes across all approved regimens.
Objective: To evaluate the cost-effectiveness of treatments for relapsed and/or refractory MM from a U.S. health system perspective.
Methods: We developed a partition survival model with 3 health states (progression-free, progression, and death) to evaluate the following regimens: carfilzomib (CFZ), elotuzumab (ELO), ixazomib (IX), daratumumab (DAR), and panobinostat (PAN) in combination with lenalidomide (LEN) or bortezomib (BOR) plus dexamethasone (DEX) in the second and/or third line of therapy. To estimate relative treatment effects, we developed a network meta-analysis and applied progression-free survival hazard ratios to baseline parametric progression-free survival functions derived from pooled data on LEN+DEX. We estimated overall survival using data on the relationship between progression-free survival and overall survival from a large meta-analysis of MM patients. Modeled costs included those related to drug treatment, administration, monitoring, adverse events, and progression. Utilities were from publicly available data and manufacturer data, if published sources were unavailable.
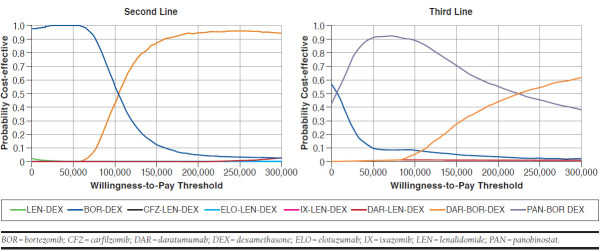
Results: Model results showed that regimens containing DAR yielded the highest expected life years (DAR range: 6.71-7.38 vs. non-DAR range: 3.25-5.27) and quality-adjusted life-years (QALY; DAR range: 4.38-5.44 vs. non-DAR range: 2.04-3.46), with DAR+BOR+DEX (second line) and PAN+BOR+DEX (third line) as the most cost-effective options (incremental cost-effectiveness ratio: $50,700 and cost saving, respectively). The applicability of the PAN+BOR+DEX result may be challenging, however, because of ongoing toxicity concerns. In the probabilistic sensitivity analysis, second-line DAR+BOR+DEX and third-line PAN+BOR+DEX had an 89% and 87% probability of being cost-effective at the $150,000 per QALY threshold, respectively.
Conclusions: The introduction of newer drugs and regimens to treat second- and third-line relapsed/refractory MM appears to provide clinical benefits by lengthening progression-free and overall survival and improving quality of life. However, only the addition of DAR or PAN may be considered cost-effective options according to commonly cited thresholds, and PAN+BOR+DEX results require cautious interpretation. Achieving levels of value more closely aligned with patient benefit would require substantial discounts from the remaining agents evaluated.
Disclosures: Funding for this work was provided in part by the Institute for Clinical and Economic Review, which collaborated on the design, conduct, and reporting of this evaluation. During the conduct of this study, Ollendorf, Synnott, Chapman, and Pearson report grants from Blue Shield of California Foundation, California Health Care Foundation, and Laura and John Arnold Foundation and also report other grants from Aetna, AHIP, Anthem, Blue Shield of California, CVS Caremark, Express Scripts, Harvard Pilgrim Health Care, OmedaRx, United Healthcare, Kaiser Permanente, Premera, AstraZeneca, Genentech, GlaxoSmithKline, Johnson & Johnson, Merck, National Pharmaceutical Council, Takeda, Pfizer, Novartis, Lilly, Spark Therapeutics, Sanofi, Prime Therapeutics, and Health Care Service Corporation outside the submitted work. Carlson reports grants from the Institute for Clinical and Economic Review during the conduct of the study and personal fees from Seattle Genetics, Genentech, and Pfizer outside the submitted work. Russo, Guzauskas, Liu, and Brouwer have nothing to disclose. Study concept and design were contributed by Carlson, Guzauskas, and Ollendorf. Guzauskas, Chapman, Synnott, and Liu collected the data, and Carlson, Guzauskas, Chapman, and Ollendorf contributed to data analysis, along with Synnott and Liu. The manuscript was written by Carlson, Guzauskas, and Brouwer, along with Chapman, Synnott, and Ollendorf, and revised by Carlson, Brouwer, and Guzauskas, along with Chapman, Synnott, and Ollendorf.
Conflict of interest statement
Funding for this work was provided in part by the Institute for Clinical and Economic Review, which collaborated on the design, conduct, and reporting of this evaluation. During the conduct of this study, Ollendorf, Synnott, Chapman, and Pearson report grants from Blue Shield of California Foundation, California Health Care Foundation, and Laura and John Arnold Foundation and also report other grants from Aetna, AHIP, Anthem, Blue Shield of California, CVS Caremark, Express Scripts, Harvard Pilgrim Health Care, OmedaRx, United Healthcare, Kaiser Permanente, Premera, AstraZeneca, Genentech, GlaxoSmithKline, Johnson & Johnson, Merck, National Pharmaceutical Council, Takeda, Pfizer, Novartis, Lilly, Spark Therapeutics, Sanofi, Prime Therapeutics, and Health Care Service Corporation outside the submitted work.
Carlson reports grants from the Institute for Clinical and Economic Review during the conduct of the study and personal fees from Seattle Genetics, Genentech, and Pfizer outside the submitted work. Russo, Guzauskas, Liu, and Brouwer have nothing to disclose.
Study concept and design were contributed by Carlson, Guzauskas, and Ollendorf. Guzauskas, Chapman, Synnott, and Liu collected the data, and Carlson, Guzauskas, Chapman, and Ollendorf contributed to data analysis, along with Synnott and Liu. The manuscript was written by Carlson, Guzauskas, and Brouwer, along with Chapman, Synnott, and Ollendorf, and revised by Carlson, Brouwer, and Guzauskas, along with Chapman, Synnott, and Ollendorf.
Figures
Comment in
-
The Authors Respond: Reframing the Value of Treatments for Relapsed Refractory Multiple Myeloma.J Manag Care Spec Pharm. 2018 Jul;24(7):712-713. doi: 10.18553/jmcp.2018.24.7.712. J Manag Care Spec Pharm. 2018. PMID: 29952702 Free PMC article.
-
Reframing the Value of Treatments for Relapsed/Refractory Multiple Myeloma.J Manag Care Spec Pharm. 2018 Jul;24(7):711-712. doi: 10.18553/jmcp.2018.24.7.711. J Manag Care Spec Pharm. 2018. PMID: 29952705 Free PMC article.
References
-
- National Cancer Institute . Surveillance, Epidemiology, and End Results (SEER) Program. Cancer stat facts: myeloma. 2016. Available at: https://seer.cancer.gov/statfacts/html/mulmy.html. Accessed November 2, 2017.
-
- National Comprehensive Cancer Network . NCCN Clinical Practice Guidelines in Oncology: Multiple Myeloma. Version 3.2016. Available at: https://www.nccn.org/professionals/physician_gls/default.aspx#site. Accessed November 2, 2017. - PubMed
-
- Neumann PJ, Cohen JT, Weinstein MC. Updating cost-effectiveness—the curious resilience of the $50,000-per-QALY threshold. N Engl J Med. 2014;371(9):796-97. - PubMed
-
- Sutton A, Ades A, Cooper N, Abrams K. Use of indirect and mixed treatment comparisons for technology assessment. Pharmacoeconomics. 2008;26(9):753-67. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
